A 𝒫𝓁𝒶𝒸𝑒 𝐹𝑜𝓇 𝐻𝑜𝓅𝑒 𝒶𝓃𝒹 𝒟𝓇𝑒𝒶𝓂𝓈 𝒶𝓃𝒹 𝐵𝑒𝓈𝓉 𝐵𝑒𝒶𝓊𝓉𝒾𝒻𝓊𝓁 𝐵𝑜𝑜𝓀𝓈 𝒶𝓃𝒹 𝒥𝑜𝓊𝓇𝓃𝒶𝓁𝓈 𝐼𝓃 𝒯𝒽𝑒 𝒲𝑜𝓇𝓁𝒹 ~
𝐼𝓃𝒸𝓁𝓊𝒹𝒾𝓃𝑔 𝓉𝒽𝑒 𝐿𝒾𝓉𝓉𝓁𝑒 𝐻𝑜𝓊𝓈𝑒 𝑜𝒻 𝑀𝒾𝓇𝒶𝒸𝓁𝑒𝓈
All books and journals by Laurel Sobol are available online at Barns and Noble bn.com
⭐️⭐️⭐️⭐️⭐️
https://m.youtube.com/playlist?list=PLhOT-ktlXXHs3D-QzjVFVlr9Lu48ndise
⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️⚪️ January 31, 2025 White House Reporters SCREAM As Press Secretary CONFIRMS Dr. Fauci Creat...
🟣🟣🟣🟣🟣🟣🟣🟣🟣🟣🟣 ⭐️⭐️⭐️
⭐️⭐️⭐️⭐️⭐️
Major Worldwide Class Action Lawsuits Now In Order To Stop, Refrain, And Abolish Forever All Government and Governing Bodies For All Countries Associated With NWO New World Order Have Failed The People Whom They Rule Over, Including USA, For Major Full Breeches of Contract With Said Countries In Violation Of All Human Rights and Plant Rights and Earth Systems Rights and Space Systems Through Manmade Apocalyptic Star Geo Weather and Disease Dispersal Warfare Global and Space Genocide ‼️
⭐️⭐️⭐️⭐️⭐️Enjoy thousands of books and journals and videos to improve, educate and thrive in times of yet more change! Organic non toxic lifestyle every day! Independently published by Laurel Sobol—
⭐️⭐️⭐️⭐️⭐️Enjoy thousands of books and journals and videos to improve, educate and thrive in times of yet more change! Organic non toxic lifestyle every day! Independently published by Laurel Sobol—
🆘‼️🆘‼️🆘‼️Must Scroll! Let there not be another preventable Alamo‼️
Ralph Steven Baric is William R. Kenan Jr. Distinguished Professor in the Department of Epidemiology, and Professor in the Department of Microbiology and Immunology at The University of North Carolina at Chapel Hill.
Fresh from his Wimbledon victory, spectators at Flushing Meadows will be denied the opportunity of seeing one of the game’s all time greats purely because the White House is continuing a discriminatory policy that has been dropped by most other major western countries.
“The U.S. Open organisers have said they would respect the Government’s rules on non-citizens being fully vaccinated in order to enter the country, ruling out Djokovic,” reports the Daily Mail.
The Serbian, who has won the US Open three times before, won’t risk traveling to the country and experiencing a repeat of his atrocious treatment by authorities in Australia, which ended up in him being deported.
Djokovic previously told the BBC that while he is not against vaccinations, he has “always supported the freedom to choose what you put in your body.”
“I’m not going to go to America if I don’t have permission, so the Australian saga for me was not pleasant at all,” he also stated.
“People still think I forced my way to Australia and tried to come in with no papers, permission or exemption – it is not true. That was proven in the court cases, so I would never go into a country where I didn’t have permission to travel,” said Djokovic.
Maybe Djokovic should just join a migrant caravan and sneak across the border, given that there are zero vaccine checks on those people entering America.
“It’s an unhappy reminder that America continues to discriminate ruthlessly against vaccinated people by banning them from visiting the country, even though its own health agencies admit that the vaccines do not prevent infection or transmission,” writes Will Jones.
A petition calling for Djokovic to be allowed to enter the states to compete at the tournament has been posted here.
As we highlighted earlier this month, following his 7th Wimbledon title victory, Djokovic vowed that he wouldn’t cave and get vaccinated simply to further his career.
⭐️⭐️⭐️⭐️Enjoy thousands of books and journals and videos to improve, educate and thrive in times of yet more change! Organic non toxic lifestyle every day! Independently published by Laurel Sobol— https://www.etsy.com/search?q=laurel%20sobol if book links are broken or no longer available then find books on Amazon. This is the home and supporter sponsor of Organic Lifestyle Today. Join over 8 billion people global in healthy creation of Elohim, our Creator. The timeless manmade Apocalyptic Star Wars with UFO technology, Geo, Weather, Disease Dispersal Warfare against Bene' Qodesh must end forevermore. People must dream, believe, hope. strive for the world and space they know is fantastical, beautiful, exotic, wonderful and miraculous --just the way our great I Am our God made it all. Soli Deo Gloria forever. ⭐️ https://m.youtube.com/playlist?list=PLhOT-ktlXXHs3D-QzjVFVlr9Lu48ndise Sponsored by Organic Lifestyle Today! ⭐️⭐️⭐️⭐️⭐️Laurel Sobol https://www.amazon.com/-/e/B006UYOMAO
🟢🔴🟢🔴🟢🔴🟢🔴🟢🔴🟢⭐️
Propagandists now try to position COVID vaccine “Novavax” as HERBAL medicine after realizing public has lost all faith in deceptive pharmaceutical industry
An internist who looked at several COVID jabs under a microscope is sounding the alarm after her discovery of strange, unidentified objects in the shots, including metallic fragments, “graphene-like” structures in each jab, and a tentacled, moving organism-like creature in the Moderna jab.
(Article by Emily Mangiaracina republished from LifeSiteNews.com)
Dr. Carrie Madej, who said she has examined the magnified contents of the Moderna, Pfizer, and Johnson & Johnson shots, found it “very upsetting” to see things in each jab that the manufacturers have not been forthright about — so upsetting that she said she cried after she verified with a second batch of shots what she had seen in the first.
She explained on the Stew Peters show that she was first asked by a local Georgia lab to examine under a microscope the contents of a “fresh” Moderna vial, which she verified was unaltered before being placed onto a glass slide under a compound microscope. “Nothing was added to the solution, nothing was diluted,” she said.
“First it looked just translucent. And then as time went on, over two hours, colors appeared. I had never seen anything like this. There wasn’t a chemical reaction happening. It was a brilliant blue, and royal purple, yellow, and sometimes green,” she said.
She later shared that when she asked nanotech engineers what the emerging brilliant colors might come from, the engineers said the “only thing they knew that could do that” was a white light, over time, causing a reaction on “a super-conducting material.” In this case, Madej noted, white light came from the microscope itself.
She pointed out that an example of a super-conducting substance would be “an injectable computing system.”
Madej went on, “These fibers were appearing more and more. Some of the fibers had a little cube structure on them, I’m not sure what that was. And also metallic fragments were in there. They were not metallic fragments I’m used to seeing.They were exotic. They were very opaque.”
In time, Madej said, “all the particulates, all these colors started moving to the edge” of the cover slide. “There was self-assembling going on, things were growing. They looked synthetic.”
Madej noticed something else quite strange: “There was one particular object or organism, I’m not sure what to call it, that had tentacles coming from it. It was able to lift itself up off of the glass slide. It appeared to be self-aware, or to be able to grow or move in space.”
She found it disturbing but said she thought, “Maybe that was a fluke in a way, maybe that was just that one vial.”
Some time later, the same lab obtained more vials from a different batch of Moderna shots, as well as a J&J vial. Madej was concerned to see the same things she had observed in the first vial.
“Another one of those tentacle-like structures appeared,” she said. “This was now completely under the cover slip, so there was no movement because it wasn’t on the edge, but I just couldn’t believe I saw another one. Same thing.” Madej also saw the “same colors” appear over time, as well as the fibers.
In the J&J vial, Madej said, there was “definitely a substance that looked like graphene. They all had graphene-like structures in there. Whether or not they were, I don’t have the capability of testing them in order to know at this lab, but that’s what they appeared to be.”
The vial’s contents also had “fatty substances, a sticky glue-like substance that would be considered a hydrogel in those, both of them.”
The J&J vial “also had colors appear.” “Their colors were different, like a fluorescent pastel kind of color. Again, a lot of synthetic structures in there as well.” Madej also noticed many “spherical ring structures” in the J&J contents.
“I’ve never seen anything like this before. They’re not supposed to be in these injections. What are they going to do to somebody? What are they going to do to a child? I started crying when I saw these the second time under a microscope, because it was confirmation of everything I saw the first time,” Madej said.
Madej again appeared on the Stew Peters show on October 20 to discuss her findings from a Pfizer jab vial as well as another J&J vial. “What I’m seeing in all of these manufacturers are synthetic substances, graphene-like, also these nano-carbon tubes,” Madej said.
“In this particular J&J” vial, Madej saw “round spheres, which were not air bubbles.” She continued, “There’s many of these rings, and as time went on they would get thinner and thinner and expand out and then finally extrude out some gelatinous material — I’m not sure what it was, but different kinds of things were inside these spheres. So they’re almost like a delivery structure, that’s what they were doing.”
On one of these rings, Madej saw what “looked like a translucent organism that went around, and back and forth.” Madej first “thought it was another water parasite,” but after continuing to observe its movements, “thought perhaps it was moving in a more robotic way.”
Madej saw the “same kind of synthetic things” in the Pfizer jab, as well as “something that looks similar to teslaphoresis. That’s when these little graphite-like black, metallic particles start to coalesce into strings, like a spider web. They do that through any external force — it could be light, it could be a magnetic force, it could be an impulse, like a frequency. Anyhow, all these little particles would then coalesce and form their own neural network, or their own fibers, or wires.”
After listening to Madej’s findings and seeing the photo and video documentation she provided, Peters commented, “It’s like I’m watching a seriously bad B-movie, a horror thriller.”
Are the Moderna jab’s tentacled creatures ‘immortal’ hydra experiments?
Madej believes the tentacled entity she found in the Moderna jabs has a connection with the organism hydra vulgaris. “It is one of the model organisms that the transhumanists like to study and look at. They feel that this is an amazing organism for humanity,” said Madej, in part because “it’s immortal in the lab setting” and “continuously produces its own stem cells.”
“It never stops. You can chop it up into little bits, put it in a petri dish and it forms itself again and again,” she continued. “They’re thinking, wouldn’t this be great if we could put this inside of a human body’s genome, and then if your hand was chopped off by a trauma, you could grow a new hand.”
The other reason the transhumanists are interested in the hydra, said Madej, is that it “has its own neural network,” that looks like a human nerve, and when [gathered together] “can form a mesh network, they actually can communicate between each other, almost like if you had your own intranet inside your body.” She noted that then “something outward could affect it, like an impulse, a frequency, something from 5G, a light, a magnet. What if something influenced that communication network?”
On October 21, Karen Kingston pointed out on the Stew Peters show that the National Institutes of Health (NIH), which owns a 50% stake in Moderna’s mRNA-1273 vaccine and it helped develop under the National Institute of Allergy and Infectious Diseases (NIAID) led by Dr. Anthony Fauci, “has been sponsoring research on hydra for more than two decades.”
In fact, the NIH has an entire subsection of its website dedicated to the Hydra 2.0 Genome Project.
Kingston also pointed to a study that found that Hydra has “about the same number of genes as humans, sharing many of the same ones,” and that they also found in the Hydra genes “linked with Huntington’s disease” and with plaque formation seen in Alzheimer’s disease. She compared the symptoms associated with these diseases with those being experienced by some who have received the COVID jabs, such as body tremors, in those who have “lost control of their neurological system.”
She believes people are being injected through the COVID shots with “transgenic hydra,” which she describes as an organism with DNA from another organism incorporated into it.
Another doctor’s ‘delivery structure’ findings in Johnson & Johnson jab
Madej is not the first to observe metallic unidentified objects, graphene-like substances, self-assembling particles, and organism-like entities in the COVID jabs.
Dr. Jane Botha reported on the Stew Peters show on October 4 that when she put a drop from a J&J shot vial under the microscope and left the droplet uncovered, she saw “very symmetrical black discs” that “seem to be joined together,” by what Peters noted appeared to be metal connectors.
Botha did not know what to make of what she was seeing, but noted that they reflected light when observed under a dark field, and that they appeared to be “self-assembling.” She saw the same discs four different times, using four different droplets from the same vial.
When the sample dried, said Botha, she could no longer see the disc structures, but “black lines started to form.”
Botha was especially disturbed by what she found because when she viewed the jab fluid through a different microscope technique, more amorphous-looking “black structures” appeared to be “exactly the same structure” that she observed in the blood of her jabbed patients who were experiencing symptoms after the COVID shots. These symptoms included blood clots, shortness of breath, nerve pain, severe thrombosis, severe embolisms, and cognitive difficulties, including memory loss and depression.
Pharmaceutical researcher Dr. Jane Ruby shared on the Stew Peters show on October 6 that people have done “reverse searches” and have “put a lot of different science together to show that this is a technology that’s called micro-bubbles,” which she says is a delivery system used for the human body.
Ruby said Dr. Botha “is hypothesizing” that the reason she could no longer see the discs, but only black lines once the J&J jab sample dried up, is that “maybe they were programmed to break open” and “spill over their contents, their payload.”
This hypothesis would correspond with Dr. Madej’s observation in the J&J jab sample of “rings” that “as time went on they would get thinner and thinner and expand out and then finally extrude out some gelatinous material,” which she described as “almost like a delivery structure.”
The International Journal of Pharmaceutical Sciences and Research has published an “overview” of “the concept of microbubble as a drug delivery system,” describing microbubbles as a “small spherical type of bubble” “capable of penetrating even into the smallest blood capillaries & releasing drugs or genes, incorporated on their surface, under the action of ultrasound.”
Repeated findings of graphene oxide-like substances in jabs
Others have observed substances in the COVID jabs that they believe to be graphene oxide, which has been shown in various experiments to have toxic effects.
The first such finding to come to prominence was the observation by Dr. Pablo Campra Madrid, published in the Spanish blog La Quinta Columna, that the contents of what was labeled as a Pfizer jab, as viewed under an electron microscope, “present[ed] a high similarity with images of graphene oxide from the literature obtained by the same TEM technique, with similar magnifications.”
They added that in both images “an intricate matrix or mesh of folded translucent flexible sheets can be observed.” The researchers concluded although the “microscopy does not provide conclusive evidence,” it “provides strong evidence for the probable presence of graphene derivatives.”
Graphene oxide, one of the many derivatives of graphene, is praised for qualities that lend themselves well to biomedical applications such as biosensors, drug delivery, and the transfer of genetic material. For example, the Science Advisory Board describes the design by researchers from the National Center for Neuroscience and Technology in China of a “hydrogel containing an RNA vaccine” that used graphene oxide, favored at least in part for its “high drug-loading efficiency” due to its “large surface area.”
In fact, a whole study has been dedicated to the “potential of graphene-based materials to combat COVID-19,” which states, “Graphene and graphene-related materials (GRMs) exhibit extraordinary physicochemical, electrical, optical, antiviral, antimicrobial, and other fascinating properties that warrant them as potential candidates for designing and development of high-performance components and devices required for COVID-19 pandemic and other futuristic calamities.”
Dr. Robert Young, a Ph.D. and naturopathic practitioner, has also examined each available COVID jab with microscopy and x-ray spectroscopy, finding objects in the Pfizer sample that bear similarity to images of graphene oxide. The microscope images and chemical/elemental content he found through x-ray spectroscopy lead him to believe the Pfizer jab contains graphene oxide.
Dr. Ruby has noted that various studies have found toxic effects of graphene oxide, including its tendency to lead to blood clotting.
A 2016 study titled “Toxicity of graphene-family nanoparticles: a general review of the origins and mechanisms has noted that “due to their nanosize, GFNs can reach deeper organs by passing through the normal physiological barriers,” such as “the blood-brain barrier and blood-placental barrier.”
The study found that “Graphene Oxide (GO) can result in acute inflammation response and chronic injury by interfering with the normal physiological functions of important organs.” “Many experiments have shown that GFNs have toxic side effects in many biological applications,” it concluded.
The Food and Drug Administration of Taiwan (TFDA)’s own official publication has also noted graphene oxide’s toxic effects.
It should be noted that the Graphene Flagship, funded by the European Union, has described one of the major developments of graphene usage as its contribution to 5G “transmitter and receivers”: “Ultra high capacity transmitter and receivers using graphene offer a unique solution to future 5G communications,” reads\ the 2018 development on the graphene timeline.
Graphene’s contribution to 5G “data transmitters and receivers” has also been discussed by the Estonian Public Broadcasting science news portal Novaator.
Birx is trying to cover for herself, Fauci, and other plandemic co-conspirators
Keep in mind that Birx and her kind initially denied the idea that covid could have come from a lab, insisting that it magically appeared in bat soup at a wet market in Wuhan.
After that narrative failed, these same folks suddenly agreed that covid could be lab-made, but that it was all just a big accident, which is the narrative that Birx is now running with.
“Someone working in the lab with one of the strains could’ve caught it and not known they had it,” Birx claims.
“In laboratories you grow the virus in human cells, allowing it to adapt more. Each time it passes through human cells, it becomes more adapted.”
Nothing that she, Fauci, or anyone else in the United States did in the aftermath of covid’s appearance was in any way wrong, Birx further contends. In her mind, China is totally to blame because they should have been testing for COVID from the beginning.
“I think the world lost several months of preparation because we were thinking there wasn’t that level of human-to-human spread when there clearly was,” Birx alleges.
China has repeatedly denied that covid leaked from a lab, calling the idea a “conspiracy theory.” And, of course, the communist regime denies any wrongdoing in how it handled the outbreak.
Early on, then-President Donald Trump suggested that covid was probably manufactured in a lab. He was mocked for saying this by the likes of Birx and others.
Since that time, Trump’s ideas have become more and more accepted, especially as it becomes increasingly clear that the entire plandemic was planned by globalists both in the U.S. and elsewhere – and Birx is one such globalist.
It turns out that Birx’s sudden appearance on the world stage is all about grifting her new memoir, which very few people will ever read. She is clearly trying to profit even more from the authoritarian monstrosity that she helped foist on the public in the name of “public health” – but will it work?
The latest plandemic-related news, including more exposés on Birx and her fellow plandemic co-conspirators, can be found at Pandemic.news.
⛔️ The Great Barrington Declaration, which condemns theplandemictyranny, was authored by Dr. Jay Bhattacharya, Martin Kulldorff and Dr. Sunetra Gupta. Both Fauci and former National Institutes of Health (NIH) head Francis Collins criticized the Declaration publicly and in private, we now know.
Will the Biden regime actually be held criminally liable for its crimes against humanity?
White House press secretary Karine Jean-Pierre also received discovery requests from the judge, as did former Disinformation Governance Board chief Nina Jankowicz; Jen Easterly, director of the Cybersecurity and Infrastructure Security Agency; and agencies including the Department of Homeland Security (DHS) and the Centers for Disease Control and Prevention (CDC).
The suit is led by Missouri Attorney General Eric Schmitt and Louisiana Attorney General Jeff Landry, who reportedly also served subpoenas to Meta, Facebook’s parent company; YouTube, which is owned by Google; Twitter; Instagram; and LinkedIn.
The subpoenas require all recipients to provide the requested documents before August 17.
Those documents reference how Jen Psaki, Jean-Pierre’s predecessor, admitted publicly back in July 2021 that officials from the regime were “in regular touch with these social media platforms” and that “we’re flagging problematic posts for Facebook that spread disinformation.”
In a statement, Schmitt said that he and Landry are committed to fighting to “get to the bottom of this alleged collusion and expose the suppression of freedom of speech by social media giants at the behest of top-ranking government officials.”
Not only the government needs to be held accountable but also the medical and pharmaceutical establishments, which also colluded with the regime and Big Tech to push deadly interventions like masks and “vaccines.”
“I am very sad for those who drank the Kool-Aid and followed the advice of people like Fauci and his corrupt organizations,” wrote a commenter at The Epoch Times.
“These people need to be held accountable for their abuse of power during the scamdemic,” wrote another.
“This is a start,” piped in someone else. “Their cumulative actions have nearly destroyed this country. Millions have died and will still die in the future as a result of their greed and bloodlust.”
The latest plandemic-related news can be found at Pandemic.news.
⭐️⭐️⭐️⭐️Enjoy thousands of books and journals and videos to improve, educate and thrive in times of yet more change! Organic non toxic lifestyle every day! Independently published by Laurel Sobol—
https://www.etsy.com/search?q=laurel%20sobol
if book links are broken or no longer available then find books on Amazon.
This is the home and supporter sponsor of Organic Lifestyle Today. Join over 8 billion people global in healthy creation of Elohim, our Creator. The timeless manmade Apocalyptic Star Wars with UFO technology, Geo, Weather, Disease Dispersal Warfare against Bene' Qodesh must end forevermore. People must dream, believe, hope. strive for the world and space they know is fantastical, beautiful, exotic, wonderful and miraculous --just the way our great I Am our God made it all. Soli Deo Gloria forever. ⭐️ https://m.youtube.com/playlist?list=PLhOT-ktlXXHs3D-QzjVFVlr9Lu48ndise
Sponsored by Organic Lifestyle Today!
⭐️⭐️⭐️⭐️⭐️Laurel Sobol https://www.amazon.com/-/e/B006UYOMAO
Despite its strong association with the federal budget, foreign aid isn’t just money. It’s anything that one country donates or provides for the benefit of another country. This can be money. However, foreign aid can also include goods, such as food or technical support. Most American foreign aid funds go through the US Agency for International Development (USAID), a semi-independent agency that manages the lion’s share of America’s development and humanitarian aid.
We’ve previously explained foreign aid, and covered some popular foreign aid myths and facts. Let’s take a look at who receives the most foreign aid, and how the US is contributing to much-needed development and humanitarian activities around the world. Broadly speaking, the US government classifies foreign as one of two categories: military aid and economic aid.
The foreign aid budget goes through several phases, beginning with the president’s budget request, and continuing through the appropriation and planning phase, obligations, and, finally, disbursements. Reporting these numbers can take some time, so we’ll look at what was actually paid out in 2023, and what the president has requested in funding for 2024.
Where we gave the most foreign aid in 2023
In 2023, the United States spent nearly $61 billion on foreign aid. Fully half of that budget has gone to just ten countries:
Where we’re budgeting the most foreign aid in 2024
The 2024 foreign aid budget was released in February, 2024. Many of these numbers can change—for example, in 2023, just under $775 million was budgeted for Syria. However, the actual disbursements increased by $121 million (in part due to the earthquake that hit Syria and Türkiye). That said, the proposed budget for 2024 is a little over $50 billion, roughly 17% less than 2023, with 20% of that budget requested for just ten countries:
Israel ($3.3 billion)
Jordan ($1,45 billion)
Egypt ($1,43 billion)
Ukraine ($774 million)
Nigeria ($625 million)
Mozambique ($564 million)
Uganda ($562 million)
Tanzania ($561 million)
Kenya ($514 million)
Zambia ($507 million)
James Nangiro Lokwatuk (31) has been part of Concern Kenya’s livestock treatment e-voucher program for the past two months. Funded by USAID, the emergency response scheme enables pastoralists to access treatment from a private sector veterinary supplies company at a reduced cost. The idea is to motivate herders to treat their animals routinely, so that they will continue to make it a priority when the scheme finishes. (Photo: Gavin Douglas / Concern Worldwide)
How are countries spending foreign assistance?
What countries do with their foreign assistance from the United States depends on what the aid is earmarked for.
For example, 25% of Jordan’s funding in 2023 was designated for military assistance. This can include a broad range of programming, from counter-terror operations to strengthening legal and judicial systems.
On the other end of the spectrum, many of the top countries for US foreign aid received overwhelmingly economic assistance in 2023. In many of these cases, the majority of economic aid has been designated for areas such as emergency response, food security, and maternal and child health.
Suliman* and his family are refugees from Syria, who lost their home in Türkiye during the February 2023 earthquake. Non-food essentials, delivered by Concern and funded by USAID, helped them to recover their losses.
Where does Concern fit in all this?
Concern Worldwide’s funding comes from a variety of sources, including the US government. The difference American foreign aid makes to the people that we work with cannot be overstated. Some achievements that have been powered by foreign aid include:
Getting children through to their second birthday
Continuous funding from USAID between 2008 and 2019 fueled Concern's Child Survival projects, which reached over 1.9 million women, children, community volunteers, and health workers in seven countries. This work was part of the largest USAID-NGO partnership for health, and the second-largest overall USAID-NGO partnership in the organization’s history.
Setting a new standard for treating malnutrition
USAID was also a key funder for Community Management of Acute Malnutrition, a pilot program that Concern co-developed 20 years ago that has now recognized by World Health Organization, UNICEF, and the World Food Programme as a best practice in child nutrition.
Training the next generation of humanitarian leaders
Another key Concern project, the National NGO Program on Humanitarian Leadership (NNPHL) was made possible in part by foreign aid, which in turn has trained dynamic and relevant training opportunities that help learners build their skills, knowledge, and confidence to take on leadership responsibilities in humanitarian organizations in order to improve the delivery of services to those in need of humanitarian assistance. Since the program began in 2019, NNPHL has received more than 4,000 applications and trained 243 humanitarians from 51 countries.
Sen. Marsha Blackburn (R-TN) said in a recent exclusive interview with Breitbart News that the Chinese Communist Party (CCP) is carrying out a malign influence operation against her due to her criticism of the party and its harm to the American people.
“It’s nothing new for me to be informed that the Chinese Communist Party is trying to carry out an adverse or malign influence campaign against me. They’ve been very active in social, on social media against me. This is something that has gone on over an extended period of time. … And this time around, they — they’re trying to spread misinformation and disinformation in my election,” she said.
Blackburn is running for re-election against challenger Rep. Gloria Johnson (D-TN) and has a 23-point lead over her, according to a recent poll conducted by the Beacon Center of Tennessee.
The senator recently released a campaign ad called “It’s Time to Break China,” in which she called for tougher measures against China. In the ad, she says:
Some say I’m too tough, that I should be more delicate. But you know what? It’s time to break some China. China stole our jobs, sent us a virus. They’re buying up our land and spying on us. I’m Marsha Blackburn, and I approved this message because we’re going to have to break a lot more China to save America.
Blackburn told Breitbart News that “people are loving” the ad, “because they can relate to it.”
“People know that China took our jobs. They know they sent us a virus. They know that they don’t take responsibility, that they don’t take their trade agreements [seriously], especially with Tennessee, [agricultural] products and exports that we have,” she said. “People know that China is part of the axis of evil and that they’re spying on our citizens. They sent a spy balloon to go sashaying across our country. They know that TikTok is something that endangers our children. So people relate to the China ad on so many different levels.”
She said she hopes after the 2024 election that Congress can get bipartisan agreement to to make certain China “keeps up their end of the deal.”
“When it comes to our trade, we also need to be firm with them and sanction them when they start throwing spy balloons across the country. We need to make certain that the divestment of TikTok takes place so that China no longer is collecting this data and information on our children. We also need to pass a bill that that disallows these Confucius Institutes and Confucius classrooms in our K through 12 schools and on our college campuses, because that is a part of China’s soft propaganda,” she said.
She said the CCP also “regularly” probes United States military bases, as well as cyberattacks hospitals.
“And not only that, I was talking with one of our hospital administrators, and they were talking about the number of hack attacks that they get, cyber attacks that they get, not only every week, but every day. And most of this is coming from China or other actors in the axis of evil, which are Russia, Iran, North Korea and China,” she said.
“China is our, our primary adversary and threat, when you look at their push to be globally dominant by the time we get to the midpoint of this century, and when you read TheHundred-Year Marathon, you see what China is up to, when you look at what they are doing through the Belt and Road Initiative and what they are doing with debt diplomacy.
“Then see what China is up to on a global basis when you see them coming into our hemisphere and entering into debt diplomacy agreements and establishing ports, you see that they’re trying to spread their footprint,” she said.
Biden Admin To Unveil Reformulated Booster Shots In September
by Zero Hedge
The Biden administration is aiming for a mid-September rollout for reformulated Pfizer and Moderna COVID-19 booster shots, after both companies promised they would be able to deliver doses by then, according to the New York Times, citing people familiar with the deliberations.
The new versions are expected to perform better against then now-dominant (yet far more mild than Delta) BA.5 Omicron subvariant, though the Times notes that data on the reformulated shots is still preliminary.
As such, federal officials have decided not to expand eligibility for the next round of existing boosters this summer – which have only been approved for Americans over 50, or those over the age of 12 who have immune deficiencies.
Dr Fauci, interestingly enough, apparently didn’t get his way, as the Times reports that he was pushing for more of the current vaccine to go into arms before the reformulated version is ready.
In internal deliberations, some senior health officials argued that eligibility for a second booster should be broadened before the reformulated version is ready because coronavirus infections are on the rise again. Dr. Anthony S. Fauci, the president’s chief medical adviser, and Dr. Ashish K. Jha, the White House pandemic response coordinator, both advocated that position. -NYT
“I think there should be flexibility and permissiveness in at least allowing” a second booster for younger Americans, Fauci told the Times earlier this month.
Another alternative under discussion was offering the shots only to a subset of younger, at-risk individuals – such as pregnant women (who don’t have periods to disrupt!).
The FDA and the CDC, however, said the government should concentrate on a fall campaign for the reformulated doses, as long as they were ready for ‘prime time’ (disregarding the typical decade of so development and safety testing for most vaccinations, of course). Both Pfizer and Moderna said millions of doses would be ready by mid-September, so regulators made the call to wait for those shots.
All adults are expected to be eligible for the updated boosters, while Children could be eligible as well according to insiders.
According to the Biden administration, anyone who is eligible for shots now should just get them as opposed to waiting for the fall – despite its reduced efficacy against Omicron vs. the original strains it was developed for.
The Times notes that “Deaths from Covid-19 are still heavily concentrated among older age groups, while hospitalizations remain well below the peak of the Omicron wave last winter.“
One concern was assuring that people did not get a booster now followed by another with the updated formulation too soon after. Officials worried that, especially for young men, two boosters in close succession might elevate the risk of a rare heart-related side effect, myocarditis, that has been linked to both Pfizer’s and Moderna’s vaccines.
For other reasons, immunologists warn against receiving booster shots in short intervals. -NYT
“You can’t get a vaccine shot Aug. 1 and get another vaccine shot Sept. 15 and expect the second shot to do anything,” said La Jolla Institute of Immunology virologist, Shane Crotty. “You’ve got so much antibody around, if you get another dose, it won’t do anything.”
“The antibodies stop that next dose from working” if the next dose is administered too early, he continued.
It will be interesting to see how many people actually get booster shots, given that federal officials are already concerned over the ‘public’s patience with additional shots,’ according to the Times, which notes that the number of people getting the jab has been dropping more with each new one offered – to the point where fewer than 30% of eligible Americans have elected to receive a second booster, which would be their fourth total shot.
To accomplish the rollout, the Department of Health and Human Services made an advance purchase of 105 million doses of Pfizer’s reformulated offering for $3.2 billion, with a possible fall deployment in mind. A similar agreement with Moderna is expected soon.
Fourth-Quarter and Full-Year 2021 Earnings Conference Call Prepared Remarks
February 8, 2022
[Slide 4: Opening Remarks – Albert Bourla]
Albert Bourla – Pfizer Inc. – Chairman and Chief Executive Officer
[Slide 5: FY 2021 Key Highlights]
[Slide 6: FY 2022 Total Company Guidance]
[Slide 7: COVID-19 Vaccinations: U.S. Patient and Economic Estimated Impact]
[Slide 8: Long-term Expectations for COVID-19]
[Slide 9: Tools to Help Manage Pandemic and Move into Endemic Phase]
[Slide 10: Bringing These Tools to the World]
[Slide 11: Maintaining Leadership in COVID-19]
[Slide 12: Pfizer's Capital Allocation Strategy (1 of 2)]
[Slide 13: Pfizer's Capital Allocation Strategy (2 of 2)]
[Slide 14: Pfizer’s mRNA Strategy Roadmap]
[Slide 15: Four Recent Agreements that Will Help Advance our mRNA Strategy]
[Slide 16: Bolstering the Pipeline with Recent Business Development Opportunities]
[Slide 17: Pfizer's ESG Strategy: Creating Value for Multiple Stakeholders (1 of 2)]
[Slide 18: Pfizer's ESG Strategy: Creating Value for Multiple Stakeholders (2 of 2)]
[Slide 19: An Outstanding Year Made Possible by Outstanding People]
[Slide 20: Scientific Updates – Mikael Dolsten] Mikael Dolsten – Pfizer Inc. – Chief Scientific Officer and President, Worldwide Research, Development and Medical
[Slide 21: Advancing Breakthroughs at the Speed of Science]
[Slide 22: PAXLOVID: Preclinical Data on SARS-CoV-2 Variants]
[Slide 23: External in vitro Data on Key Therapeutics Against Variants]
[Slide 24: PAXLOVID: Target Populations for Clinical Studies]
[Slide 39: Danuglipron (Oral GLP-1): Phase 2 Study in Type 2 Diabetes]
[Slide 40: Key 2H 2021 Achievements and 2022 Potential Milestones]
[Slide 41: Financial Review – Frank D’Amelio]
Frank D’Amelio – Pfizer Inc. – Executive Vice President, Chief Financial Officer
[Slide 42: Quarterly Income Statement Highlights]
[Slide 43: 2021 Financial Guidance vs. Results]
[Slide 44: 2022 Financial Guidance]
[Slide 45: Capital Allocation Framework]
[Slide 46: Key Takeaways]
Risks Related to Our Business, Industry and Operations, and Business Development:
Risks Related to Government Regulation and Legal Proceedings:
Risks Related to Intellectual Property, Technology and Security:
Fourth-Quarter and Full-Year 2021 Earnings Conference Call Prepared Remarks
February 8, 2022
[Slide 4: Opening Remarks – Albert Bourla]
Albert Bourla – Pfizer Inc. – Chairman and Chief Executive Officer
[Slide 5: FY 2021 Key Highlights]
2021 was a watershed year for Pfizer. A year in which we set all-time highs in all major areas of focus for Pfizer.
• We reached an estimated 1.4 billion patients with our medicines and vaccines. That’s more than one out of every six people on Earth. Never before has Pfizer’s patient impact been so widereaching.
• We improved our ranking from fourth to second among large biopharma companies in the PatientView Global Survey.
• According to Morning Consult, 61% of Americans have a favorable view of Pfizer, which is up 33 points since January 2020.
• Just last week, Fortune ranked us fourth on its annual World’s Most Admired Companies list – the highest ranking we have ever achieved.
• Ninety-five percent of our colleagues said in an internal survey that they are proud to work for Pfizer, which ranks among the best in corporate America.
• We increased our investments in Research & Development (R&D) from $8.9 billion in 2020 to $10.5 billion in 2021.
• We initiated 13 pivotal clinical studies – the highest number ever for Pfizer.
• Lastly, we grew revenues by 92% operationally to $81.3 billion and Adjusted Diluted EPS by 92% operationally to $4.42.
Our successes in leading the fight against COVID-19 have not only made a positive difference in the world; I believe they have fundamentally changed our company and our culture forever. Colleagues across Pfizer are inspired by what we have achieved and more determined than ever to be part of the next potentially game-changing breakthrough. To that end, we are applying the “lightspeed” principles developed for our COVID-19 work to our other therapeutic areas to make sure we continue to move at the speed of science for the benefit of patients.
[Slide 6: FY 2022 Total Company Guidance]
As a result, we believe we can do even better with each of these metrics in 2022. Our full-year 2022 financial guidance, for example, includes for the first time ever a forecasted revenue midpoint that is $100 billion and an Adjusted Diluted EPS midpoint of $6.45.
[Slide 7: COVID-19 Vaccinations: U.S. Patient and Economic Estimated Impact]
While Comirnaty is having a significant positive impact on Pfizer’s financial performance, it’s the tremendous impact that COVID-19 vaccines have had on society that is most important. In the U.S. alone, the COVID-19 vaccination program is estimated to have saved more than one million lives and prevented more than ten million hospitalizations, according to a December 2021 Commonwealth Fund report.
The economic impact is equally astounding. According to a December 2021 Heartland Forward report, the rapid deployment and wide availability of COVID-19 vaccines in the U.S. created an estimated economic savings of $438 billion in 2021, which amounted to U.S. GDP being 2.3% higher than it otherwise would have been.
I’m proud to say that Pfizer contributed significantly to these benefits given that approximately 6 out of 10 doses administered in the U.S. as of February 6, 2022, were Comirnaty.
This is the value of our science … what our culture has enabled … and what drives our people.
Now I would like to speak to three factors that will help drive our growth going forward:
• the long-term outlook for COVID-19 and why we believe we are well positioned to continue to lead the battle against this disease;
• our thoughtful capital allocation strategy and why we believe it can help drive our growth in the second part of the decade; and
• how our commitment to ESG principles is designed to create sustainable growth for Pfizer and deliver meaningful value to patients.
[Slide 8: Long-term Expectations for COVID-19]
Let me start with the COVID-19 pandemic.
Our scientists continue to monitor the SARS-CoV-2 virus and believe it is unlikely that it will be fully eradicated in the foreseeable future. They believe this for several reasons:
• The global distribution of the virus makes it difficult to contain.
• The virus has shown an ability to mutate often, making it difficult to stay ahead of it.
• And the data appear to show that natural infections do not lead to the type of durable protection needed to prevent all transmissions and viral mutation. As a result, people can become reinfected by the same or different strains over time.
[Slide 9: Tools to Help Manage Pandemic and Move into Endemic Phase]
That said, we now have the tools – in the form of vaccines and treatments – that we believe will help enable us to not only better manage the pandemic, but also help countries move into an endemic phase. In other words, we believe these tools will help allow us to go back to normality and spend time with family and friends, travel, attend indoor dining and concerts, and enjoy many other activities while lowering the risk of overburdening hospitals and healthcare systems around the world.
[Slide 10: Bringing These Tools to the World]
All of us at Pfizer are extremely proud of the role we have continued to play in bringing these tools to the world.
• Throughout 2021, we continued our efforts to bring our COVID-19 vaccine to more populations and to further ramp up our manufacturing and distribution capabilities. As a result, the market share of our Comirnaty vaccine has continued to grow, representing 70% of all doses distributed across the U.S. and EU as of February 5.
• When it comes to Paxlovid, we expect to produce six million treatment courses during the first quarter of 2022. Overall, we expect to produce 30 million courses in the first half of 2022 and 120 million courses for the full year, depending on the global need. Having recently received a conditional marketing authorization from the European Medicines Agency (EMA), Paxlovid has now received emergency or conditional authorization for use with certain populations in approximately 40 countries so far. We are in discussions with governments around the world and expect that as the number of authorizations increase, so will the number of contracts for this treatment, which could truly be a game changer.
[Slide 11: Maintaining Leadership in COVID-19]
At Pfizer, we are keenly aware of our responsibility to continue to invest in R&D to maintain our leadership in providing these tools and other meaningful solutions to the world. That’s why we continue to develop and test different versions of our vaccine to potentially address variants of concern as they emerge, and why we are currently working on a new omicron-based vaccine candidate and on a bivalent COVID-19 vaccine candidate. It’s also why just two months after receiving Emergency Use Authorization (EUA) from the U.S. Food & Drug Administration (FDA) for Paxlovid, we are already working on a potential next-generation oral COVID-19 treatment.
Going forward, we are confident in our ability to maintain this leadership position because of our significant investments in R&D combined with our ability to move at the speed of science without compromising quality or safety; the strong credibility we have earned with governments, healthcare providers and consumers combined with our extensive global field presence; and our unparalleled capabilities for highquality manufacturing at scale.
[Slide 12: Pfizer's Capital Allocation Strategy (1 of 2)]
The second thing I wanted to touch on is how we think about our capital allocation and to repeat once more our strategy.
We feel that the entirety of our business continues to demonstrate a robust topline growth trajectory through 2025. Consensus estimates are beginning to slowly recognize this momentum.
However, consensus estimates currently show our topline shrinking from 2025-2030. This is inconsistent with our own plans. Our goal is to continue to be a growth company from 2025-2030, despite the impact of LOEs expected during that period.
Our confidence in this is underpinned by the momentum of our business, the durability of our COVID-19 offerings as I just described, the underestimated strength of our internal pipeline, and, of course, by our ability to deploy capital into growth-focused business development to access external science.
[Slide 13: Pfizer's Capital Allocation Strategy (2 of 2)]
We leverage business development opportunities to advance our business strategies and objectives. The strength of our balance sheet and cash flows allows us to pursue new business development opportunities going forward that could add at least $25 billion of risk-adjusted revenues to our 2030 topline expectations. We expect to do this while still maintaining our growing dividend, as well as flexibility for other uses of our cash.
The focus of our business development efforts will continue to be on compelling external science in the form of both later-stage assets, as well as earlier medical innovations, that have the potential to be breakthroughs for patients. Our focus will largely be in the therapeutic areas and platforms where we have the scientific skills and acumen to add substantial value and select the most successful targets. In addition, we feel that we have distinctive attributes such as world-class excellence in clinical development and unsurpassed manufacturing and commercial capabilities at scale that make us a very attractive partner across a variety of deal arrangements. We believe the opportunities to deliver on this approach exist, and I will be personally focusing on its execution.
I want to emphasize that despite our significant capital flexibility, we will never lower the scientific and financial standards we apply in our business development. As we pursue these opportunities, we will continue to be highly disciplined in our evaluation and prioritization processes.
Since 2019, we have already invested almost $25 billion in business development transactions adding more than $13 billion in consensus 2030 revenue. I would point out that the $13 billion of consensus currently includes nothing for the Trillium assets, the Biohaven collaboration, or the recently announced mRNA deals, all of which have substantial potential. I see this pace of business development accelerating going forward, and I am confident it will be an important driver in ensuring Pfizer as a growth company in the back-half of this decade.
One highly visible example of our approach to business development is the recent investments we are making in mRNA technology and collaborations.
[Slide 14: Pfizer’s mRNA Strategy Roadmap]
mRNA has emerged as a versatile technology, with potential applications across many infectious diseases, cancer, rare genetic disorders and even auto-immune diseases. Although mRNA is not the holy grail, we believe the technology has the potential to have a game-changing impact on global health, which is why we have developed a robust mRNA strategy and are aggressively building our platform.
While the pandemic has demonstrated that it’s not that easy to deliver mRNA vaccines at scale, Pfizer has emerged as a leader in this space. With decades of experience on our side, we’ve developed what is arguably the most efficient clinical development and vaccine manufacturing capabilities the world has ever seen. We also have rapidly scaled and built out new capabilities in record time by hiring nearly 2,400 new colleagues in these functions in a nine-month timeframe. Going forward, we plan to continue to invest to capitalize on the leadership we have built in terms of both mRNA R&D and manufacturing.
[Slide 15: Four Recent Agreements that Will Help Advance our mRNA Strategy]
In addition to these internal investments and improvements, we’re also making external investments to build out our capabilities in this space. For example, Pfizer recently has entered into four important business development deals to help advance our mRNA strategy.
• We are expanding our collaboration with BioNTech to use the existing platform to co-develop an mRNA vaccine candidate for Herpes Zoster Virus to protect against shingles.
• Our agreement with Beam Therapeutics expands our mRNA efforts to another core therapeutic area for Pfizer – rare disease – with a four-year research collaboration for three targets for rare genetic diseases of the liver, muscle and central nervous system. We believe this will give us the potential to use mRNA to treat diseases – not just help prevent them.
• Our agreement with Acuitas gives us the ability to collaborate with – and license – their proprietary lipid nanoparticle (LNP) technology for up to ten targets for mRNA vaccines and therapies. We believe this will give us greater independence in this space.
• And we have signed a strategic collaboration and licensing agreement with Codex DNA, a leader in the development of automated solutions for on-demand synthesis of genes and mRNA, potentially allowing enzymatic assembly of DNA at the front-end of the mRNA production process. This could possibly reduce the time to produce a new vaccine from 3 months down to 2 months. If successful, this would be an important differentiator when developing a vaccine for the flu, for example, as it would allow us to select a strain much closer to the start of any flu season.
These deals represent only four pieces of a much bigger strategic puzzle. As we continue executing on our mRNA strategy, you should expect to see more targeted activity in this area.
[Slide 16: Bolstering the Pipeline with Recent Business Development Opportunities]
Of course, our business development activity in the last quarter went beyond executing on our mRNA strategy. This is an update of the slide I showed you last quarter, and I would like to highlight a few of the other recent deals.
The acquisition of Trillium builds on our strong track record of leadership in Oncology, enhancing our hematology portfolio as we strive to improve outcomes for people living with blood cancers around the globe.
Our strategic collaboration with Biohaven leverages our leading commercial capabilities in pain and women’s health with Biohaven's groundbreaking oral CGRP receptor antagonist -the only one approved in the U.S. for both acute and preventative treatment of migraine -to potentially bring a valuable new treatment option to patients living with this debilitating neurological disease outside the U.S.
Through the proposed acquisition of Arena we plan to leverage Pfizer’s leading research and global development capabilities to accelerate the clinical development of etrasimod for patients with immunoinflammatory diseases.
[Slide 17: Pfizer's ESG Strategy: Creating Value for Multiple Stakeholders (1 of 2)]
Now, I'd like to share some details about Pfizer’s enhanced ESG strategy. The strategy is focused on six areas where we see opportunities to create a meaningful and measurable impact over the next decade: product innovation; equitable access and pricing; product quality and safety; diversity, equity and inclusion; climate change; and business ethics.
[Slide 18: Pfizer's ESG Strategy: Creating Value for Multiple Stakeholders (2 of 2)]
Each quarter going forward, I will provide examples of how we are embedding ESG into all core areas of our business. This quarter, I will highlight our efforts to:
• improve clinical trial diversity,
• improve diversity within our colleague base, and
• help ensure equitable access to our COVID-19 vaccine and treatment.
Last year, Pfizer published an industry-first retrospective analysis of demographic data of U.S. participants in 213 of our interventional clinical trials that initiated enrollment from 2011 through 2020. The analysis demonstrated that overall trial participation of Black or African American individuals was at the U.S. census level (14.3% vs. 13.4%), participation of Hispanic or Latino individuals was below U.S. census (15.9% vs. 18.5%), and female participation was at U.S. census (51.1% vs. 50.8%).
We published this analysis to be transparent and for it to serve as a baseline as we measure progress in this area. We believe that diversity in trials is a matter of equity and good science and are taking decisive steps designed to improve diversity in our trials. Our goal is to achieve racially and ethnically diverse participation at or above U.S. census or disease prevalence levels (as appropriate) in all our trials.
The second item I want to highlight is the significant progress we are making in diversifying our colleague base, particularly at more senior-level positions. In the last three years, for example, we have increased the percentage of women at the vice president level and above globally from 32% to 42%. Over that same timeframe, we have increased the percentage of minorities at the vice president level and above in the U.S. from 19% to 25%.
The third item I wanted to highlight is the progress we are making to help ensure our COVID-19 vaccine and oral treatment are accessible by everyone everywhere. I am thrilled to say that we remain on track to meet or exceed our goal of delivering at least two billion doses of our vaccine to low-and middle-income countries by the end of 2022 – having just met our goal of delivering the first one billion by the end of 2021. I also want to highlight two data points about our two billion-dose commitment.
• One billion of these doses are being provided to the poorest countries completely free of charge thanks to our agreement with the U.S. government. Pfizer is providing these doses to the U.S. government at a not-for-profit price, and the government is then providing them to the poorest countries for free.
• Also, the one billion doses we delivered in 2021 represented 37% of all doses we delivered last year.
In terms of our oral COVID-19 treatment, we have signed a voluntary license agreement with the Medicines Patent Pool (MPP), which we hope will lead to expanded access pending country regulatory authorization or approval, in 95 low-and middle-income countries that account for approximately 53% of the world’s population.
Lastly, I'm pleased to announce that the Compensation Committee of our Board of Directors has been reviewing methods for linking executive compensation with ESG performance, which we expect to begin this year.
For details regarding the impact of our ESG strategy had on our business in 2021, please keep an eye out for Pfizer’s 2021 ESG Report, which will be published online in mid-March.
[Slide 19: An Outstanding Year Made Possible by Outstanding People]
In summary, 2021 was an outstanding year for Pfizer, and we look forward to continuing to apply the lessons learned from COVID to deliver breakthroughs for patients across all our therapeutic areas. We remain focused on being nimble, investing in our R&D organization and exploring dynamic partnerships that will enable us to fully realize the power of our science.
None of this is possible without the contributions of our amazingly purpose-driven colleagues, who continue to rise to the challenge of addressing the world’s most devastating diseases. In 2021, our colleagues exceeded expectations. Therefore, we will once again use a part of the bonus pool that the Board approved for bonus-eligible colleagues to provide a one-time, special COVID-19 Circumstances Bonus (CCB) to our non-bonus eligible colleagues to reward them for their hard work and to help them cover personal, family and living expenses incurred because of the COVID-19 pandemic.
With that, I will turn it over to Mikael to update you on our R&D efforts. After Mikael, Frank will provide financial details on the fourth quarter and our outlook for 2022.
[Slide 20: Scientific Updates – Mikael Dolsten] Mikael Dolsten – Pfizer Inc. – Chief Scientific Officer and President, Worldwide Research, Development and Medical
Thank you, Albert. I’m delighted to share updates from this quarter as we continue to deliver first-in-class science.
[Slide 21: Advancing Breakthroughs at the Speed of Science]
Today, I will share updates from our COVID-19 programs and select other assets in our pipeline.
[Slide 22: PAXLOVID: Preclinical Data on SARS-CoV-2 Variants]
Let’s start with PAXLOVID.
As the COVID-19 pandemic continues to burden public health, we have advanced the science on our novel oral antiviral therapeutic.
Importantly, we see consistent, potent antiviral activity in vitro against all current variants of concern, including both Delta and Omicron.
This would be expected from how the compound was designed. On the left, you can see a crystal structure showing how tightly nirmatrelvir binds into the active site of the Omicron variant.
History has told us from the HIV protease field that the closer the therapeutic is designed to mimic the substrate, the harder it is for resistance to emerge. That combined with the essential nature of the protease, the short duration of treatment and the co-dosing with ritonavir to drug exposures that are over five to six times the amount of compound needed to kill the virus in an in vitro assay, suggests there is a reduced risk for resistance.
[Slide 23: External in vitro Data on Key Therapeutics Against Variants]
External data support our findings. Nirmatrelvir maintains in vitro potency in the low nanomolar range, as you can see in these graphs that include other authorized or approved therapeutics.
On the left is in vitro data from a study done in collaboration with the Icahn School of Medicine at Mount Sinai. Nirmatrelvir demonstrated potent antiviral activity as measured by IC50 – a measure of drug efficacy indicating the concentration needed to inhibit infection by half.
This is consistent with findings from the Rega Institute at KU Leuven in Belgium, shown on the right.
[Slide 24: PAXLOVID: Target Populations for Clinical Studies]
We anticipate a New Drug Application decision by the FDA in the high-risk population in the second half of 2022, pivotal readouts of our household contact and standard risk studies in the second quarter and second half of 2022, respectively, and a study start in children aged 6 to 18 years old in the first quarter of 2022.
In the standard risk study, we are expanding enrollment by 750 non-hospitalized patients with symptomatic COVID-19, and vaccinated, standard-risk patients may also be eligible, provided their last SARS-CoV-2 vaccine dose was received at least 12 months prior to screening.
This expansion will allow us to further evaluate the secondary endpoint seen in the interim analysis, which showed a 70% reduction in hospitalization and no deaths compared to placebo.
We also are advancing work on a potential next generation SARS-CoV-2 antiviral with the aim of achieving similar high clinical efficacy and pan-coronavirus design properties that maintain activity, with a favorable safety profile, and counter potential viral resistance—but without the need for ritonavir boosting.
A first in human study start is expected in the second half of 2022.
[Slide 26: COMIRNATY: Pediatric (6 months through 4 years) Update]
We also continue to advance vaccine development and have achieved emergency use authorizations for use in children as young as age five.
Effectiveness data for three doses of the vaccine for people 12 years and older, and early laboratory data observed with Delta and other variants of concern—including Omicron—suggest that people vaccinated with three doses of COMIRNATY may have a higher degree of protection against both symptomatic and severe outcomes compared to two primary doses.
Informed by these data, in addition to the immunobridging data, we are evaluating a third 3 µg dose in our study of children 6 months through 4 years of age, with the belief that a third dose may be optimal for this age group.
However, as pediatric cases and hospitalizations are at an all-time high, FDA urged us to start a rolling Emergency Use Authorization submission with the two-dose efficacy, immunogenicity and safety data we have accumulated thus far while we continue to collect data, including from third-dose administration.
We plan to submit third-dose data once they are available.
In the meantime, FDA has scheduled an Advisory Committee meeting for February 15 to consider the twodose data collected to date.
If emergency use authorization of two doses is granted and the Centers for Disease Control and Prevention recommends usage, parents will have the opportunity to begin a COVID-19 vaccination series for their children between 6 months and 4 years of age while awaiting potential authorization of a third dose..
[Slide 27: COMIRNATY: Rise of Neutralizing Titers Against Omicron After 3rd Dose]
Turning to the adult population, in the wake of surging Omicron cases, in January we completed a laboratory analysis of the effect of a third dose boost of COMIRNATY on live virus neutralization.
Encouragingly, there was a more than 25-fold increase in Omicron live virus neutralizing titers observed between day of dose three and one month post-dose three.
We observed a moderate 4-month post-dose three antibody decay for Wild Type and the Omicron variant.
Between one month and four months post-dose three, neutralizing titers were 1.6-and 2-fold lower for Wild Type and the Omicron variant, respectively.
We’re now starting to see effects of a third dose boost in maintaining a high level of protection against Omicron in the real world.
These data from Kaiser Permanente Southern California show Omicron-related emergency department visits without hospitalization on top, and hospitalizations on the bottom.
Three doses of COMIRNATY provided better vaccine effectiveness against Omicron than two doses, and there was high vaccine effectiveness of three doses against Omicron-related hospitalization, similar to Delta-related hospitalization.
We did see some waning of effectiveness against emergency department admissions due to Omicron three months or more after a third dose, which suggests the potential need for another boost of the current vaccine or an Omicron-based vaccine.
[Slide 29: Omicron-Based Vaccine Candidate Study]
We have started an Omicron-based vaccine candidate trial in adults 18 to 55 years of age. The study will evaluate more than 1,400 participants across three cohorts:
a. Those who have already received two doses of the current vaccine 90-180 days prior to enrollment will receive one or two doses of the Omicron-based vaccine;
b. Those who have already received three doses of the current vaccine 90-180 days prior to enrollment will receive one dose of the current vaccine or the Omicron-based vaccine; and
c. Those who are vaccine-naïve will receive three doses of the Omicron-based vaccine.
This study is part of our science-based approach to develop a variant-based vaccine that we hope achieves a similar level of protection against Omicron as the current vaccine has with both Wild Type and earlier variants, but with potentially longer duration of protection.
[Slide 30: CDK2/4/6 Inhibitor: Phase 1 Study Subset in HR+ Metastatic Breast Cancer]
Now, let’s turn to our next generation CDK inhibitors.
Most patients with advanced or metastatic breast cancer eventually develop resistance to both endocrine therapy and CDK4/6 inhibitors despite their transformative efficacy.
Inhibition of CDK2, delivered as a CDK2 selective active drug or a triple activity CDK 2/4/6 agent, may prevent, delay, or reverse resistance and prolong survival.
These are data from a subset in the CDK2/4/6 inhibitor Phase 1 dose escalation and antitumor activity study of heavily pre-treated patients with hormone receptor positive metastatic breast cancer.
The most improvement in terms of tumor size reduction was seen in patients treated with monotherapy or in combination with fulvestrant.
We observed three confirmed partial responses and three patients with stable disease for more than 12 months.
One patient has been receiving ongoing treatment for more than 28 months.
There has been an acceptable safety profile at the recommended Phase 2 dose, which is 25mg twice daily.
We plan to conduct a Phase 1 dose expansion and expect to complete it in the fourth quarter of 2022.
[Slide 31: CDK2 Inhibitor: Phase 1 Study in Breast Cancer]
Selective CDK2 inhibition may allow dose titration and has the potential to be used in combination with approved CDK inhibitors, such as palbociclib, or other next-generation CDK4 selective inhibitors.
There were two confirmed partial responses in the Phase 1 study of our selective CDK2 inhibitor in patients with advanced or metastatic HR+/HER2-breast cancer who had received/progressed on prior CDK4/6 inhibition and endocrine therapy.
One patient had a maximum tumor shrinkage of 54% following CDK2 inhibitor treatment for approximately 8 months, and the second had 100% shrinkage of all target lesions following treatment for approximately 9 months.
We are showing scans of the first patient at baseline and 8 weeks.
There was an acceptable safety profile as a monotherapy, and we are currently exploring combinations.
We expect the Phase 1/2 study to be completed in the second quarter of 2023.
Now, let’s turn to our six-valent Lyme disease vaccine candidate which we are developing in partnership with Valneva.
We have received further positive data from our Phase 2 proof of concept study and expect to start Phase 3 in the third quarter of 2022 with a dosing regimen of 0, 2, and 6 months to prime, followed by routine boosters before the start of a Lyme season.
Our Phase 2 study is continuing and includes a pediatric population aged 5 to 17 years.
[Slide 33: Lyme Vaccine: Phase 2 Data]
Since Lyme disease is seasonal, our goal is to establish a regimen that results in high antibodies at the beginning of each season. We therefore looked at a boost one year after the primary series.
We saw substantial boost antibody response in Phase 2 to all six serotypes present in North America and Europe following the three-dose primary series vaccination schedule, with a 14-to 31-fold rise in season one and a 51-to 69-fold rise in season two.
The vaccine candidate was generally well tolerated at all dose levels tested, and we are excited about further development and the potential to help prevent this debilitating disease.
Last quarter, we told you that we saw robust dystrophin expression out to one year in our Duchenne Muscular Dystrophy gene therapy Phase 1b study. I will show you encouraging functional motor data in a moment.
We recently shared some very sad news that a DMD patient with advanced disease in the non-ambulatory cohort of the Phase 1b trial passed away after presenting with hypovolemia and cardiogenic shock.
This patient was 16 years old and the first in the non-ambulatory cohort treated with Rapamune, along with steroids, as part of the immunosuppressive regimen. Rapamune is not used in the Phase 3 ambulatory study. Like most non-ambulatory DMD patients, he had more advanced disease with underlying cardiac dysfunction. There is evidence of an active viral infection and we are investigating how this may have contributed to the outcome.
Additional assessment will be required to define the steps needed to re-start the Phase 1b study in nonambulatory patients who are more progressed in the disease.
I will now share the encouraging data we have seen from the ambulatory cohort of the Phase 1b study.
[Slide 35: Fordadistrogene movaparvovec: Phase 1b Ambulatory Population at 1 yr.]
Nineteen patients were enrolled, 16 of whom received the dose selected for our Phase 3 program and three of whom received a previously studied lower dose.
At one year post-treatment, there was a mean 5.6 point improvement in ambulatory function as measured by North Star Ambulatory Assessment compared to an external control, matched for age and baseline function.
This is particularly encouraging given that patients at this age and stage of disease typically experience a considerable decline in ambulatory function as illustrated by the external control.
On the right, we show time in study, with six participants nearing or more than three years since treatment.
The ambulatory cohort in Phase 1b is similar, but slightly older on average, to the population in the Phase 3 CIFFREO trial.
Considering the favorable benefit to risk profile we have seen in the ambulatory patient population and in consultation with the Data Monitoring Committee, we believe the safety profile of our DMD gene therapy is manageable in this patient group.
Additional mitigations are being added to our study protocol in consultation with the eDMC and other medical experts.
Pending regulatory feedback, we anticipate Phase 3 study sites to begin to re-open in the next few months, with the potential to report topline results and, subject to clinical trial success, submit a BLA by the end of 2023.
[Slide 36: Anti-GDF-15 mAb (ponsegromab, PF-06946860): Cancer Cachexia]
Turning now to Internal Medicine, and ponsegromab, our candidate for cachexia due to cancer.
It targets GDF-15, which is frequently elevated in cancer patients, drives reduction of appetite and body weight loss, and is associated with poor outcomes. There may also be potential to treat cachexia associated with other chronic diseases such as heart failure and COPD.
We have encouraging Phase 1b data which I will show next.
[Slide 37: Anti-GDF-15 mAb: Phase 1b (Preliminary Data) in Cancer Cachexia]
Ponsegromab was evaluated in ten cancer patients who were undergoing anti-tumor treatment and had more than 5% body weight loss in the last 6 months, or more than 2% body weight loss with a body mass index of less than 20 kg per meters squared or diagnosed sarcopenia.
Ponsegromab administration was found to suppress circulating GDF-15 levels in cancer cachexia patients below the level observed in healthy subjects.
Preliminary data from the Phase 1b trial show ponsegromab treatment resulted in significant body weight gain compared to historical placebo. You can see that the nice trend in body weight increase remained even after the dosing was stopped at week 12. The gray dotted line indicates the historical cut-off associated with improved survival.
We are co-developing a companion diagnostic with Roche Diagnostics designed to enable precision medicine, and we expect to start a Phase 2 study in cancer cachexia in the fourth quarter of 2022.
Injectable GLP-1 receptor agonists offer potent lowering of glucose and weight in diabetic and obese patients, with proven cardiovascular benefit, but this drug class is underutilized due to its injectable administration route.
Our small molecule GLP-1 receptor agonist danuglipron could potentially offer a convenient oral alternative to injectables and is being evaluated for the treatment of Type 2 diabetes, obesity and NASH.
It has been developed in our Internal Medicine research group with a vision to expand the use of this potent, easily administrated GLP-1 drug class to a primary care setting.
[Slide 39: Danuglipron (Oral GLP-1): Phase 2 Study in Type 2 Diabetes]
Here are data from the Phase 2 study in Type 2 Diabetes.
We recorded strong dose-dependent reductions in both HbA1c—a measure of long-term blood sugar levels—and body weight, compared to the marginal effects noted with placebo.
After 12 weeks of treatment with the 200 mg twice daily dose, HbA1c decreased by almost 1.6% and body weight decreased by 5.4 kilograms.
The safety and tolerability profile is consistent with the GLP-1 class and the most frequent adverse events were GI-related.
We expect to start a Phase 2b titration optimization study mid-2022 with doses up to 200 mg twice a day, and complete a Phase 2b study in non-diabetic subjects with obesity in the first quarter of 2023.
[Slide 40: Key 2H 2021 Achievements and 2022 Potential Milestones]
Here are select recent and potential upcoming milestones from across the pipeline.
The solid blue dots represent milestones achieved and the open blue dots represent anticipated milestones.
Programs in bold are major anticipated events.
Some of the programs on the right have already been designated as lightspeed, meaning they have accelerated development timelines, or are being considered for lightspeed designation.
Finally, I would like to take a moment to thank Morrie Birnbaum, our outgoing Chief Scientific Officer of the Internal Medicine Research Unit, for his immense contributions over the last seven years, and welcome Bill Sessa, who joins us from Yale School of Medicine following a decades-long career in academia—including serving as Vice Chair of Pharmacology, Professor of Medicine, and Director of the Vascular Biology & Therapeutics Program at Yale.
Bill is an eminent leader in this field, a groundbreaking scientist and a celebrated innovator, and I know he will bring his tremendous vision and insights to our investigation of cardiovascular and metabolic diseases.
Thank you for your attention and I look forward to your questions. Now, let me turn it over to Frank.
[Slide 41: Financial Review – Frank D’Amelio]
Frank D’Amelio – Pfizer Inc. – Executive Vice President, Chief Financial Officer
[Slide 42: Quarterly Income Statement Highlights]
Thanks, Mikael. I know you’ve seen our release, so let me provide a few highlights regarding the financials.
The COVID-19 vaccine once again had a significant positive impact on our quarterly results and Albert and Mikael have already addressed the key points on the COVID-19 landscape.
Turning to the income statement. Revenue increased 106% operationally in the fourth quarter of 2021 driven by COVID-19 vaccine sales and strong performance from a number of our other key growth drivers.
And looking at the revenue excluding the COVID-19 vaccine direct sales and alliance revenues and Paxlovid contribution, the fourth quarter was slower than the first nine months of the year, declining by 2% operationally. As we discussed during our third quarter call, there was a 4% negative impact, or approximately $500 million, from fewer selling days in the US and International. Excluding that impact, operational growth would have been 2%, which is still lower than the mid-to-high single digit growth we had experienced during the rest of the year.
This was factored into our forecasts for the year but let me briefly walk you through this. In our Biopharma business, you will remember that the fourth quarter of 2021 faced a tough comp from the fourth quarter of 2020 for Prevnar, as pneumococcal vaccinations were strong ahead of COVID-19 vaccine availability. Excluding vaccines from the current and comparable period would add 5 percentage points to the growth.
Adjusting for the unusual comparative period differences related to Vaccines and selling days, our revenue growth would have been approximately 7 percent, which is similar to what we've been delivering lately.
For the year, operational revenue growth was 92%. Excluding Comirnaty direct sales and alliance revenues and Paxlovid, 2021 operational revenue growth was 6%. This is consistent with our projected revenue CAGR of at least 6% from 2020 through the end of 2025. Of course, there will be some variability in quarterly and annual growth rates due to a variety of factors, but we continue to expect at least a 6% CAGR through 2025.
The Adjusted cost of sales increase shown here reduced this quarter’s gross margin by approximately 16 percentage points compared to the fourth quarter of 2020, which is almost entirely driven by the impact of the COVID-19 vaccine.
Adjusted SI&A expenses in the fourth quarter increased primarily due to increased product-level spending, including Comirnaty, including higher healthcare reform sales-based fees.
The increase in Adjusted R&D expense this quarter was primarily driven by increased investments in latestage pipeline projects, including additional spending related to our oral COVID-19 treatment.
The growth rate for reported diluted EPS was +293%, while Adjusted diluted EPS grew +152% for the quarter.
Foreign exchange movements resulted in a negative 1% impact to revenue as well as a 4% benefit, or $0.02, to Adjusted diluted EPS.
[Slide 43: 2021 Financial Guidance vs. Results]
As you can see, we achieved or exceeded each of the components of our 2021 financial guidance.
[Slide 44: 2022 Financial Guidance]
Let’s move to our first time 2022 guidance.
We’ve again provided total-company guidance, which includes the business with the COVID-19 vaccine. We will continue to provide insight into our expected revenues for Comirnaty, and, now for the first time, we will also provide some color on our expected revenues for Paxlovid. However, note that we will no longer be providing EPS guidance for the business excluding Comirnaty. Similarly, we won't provide EPS guidance for Paxlovid.
Our revenue guidance represents a record for Pfizer, and we expect total company revenue to be in a range of $98.0 to $102.0 billion, representing an operational growth rate of 24% at the mid-point. Please consider that this revenue range reflects approximately $1.1 billion of anticipated negative impact from changes in foreign currencies and also the impact of the loss of Meridian's sales of approximately $300 million, both of which your models may not take into account.
Regarding our COVID-related revenues, we now expect the COVID-19 vaccine revenue for the year to be approximately $32 billion, an increase of approximately $1 billion compared to our prior guidance provided on December 17. For Paxlovid, we expect sales of approximately $22 billion.
This means that excluding the COVID-related revenues, we expect sales to be $46 billion at the midpoint, representing operational growth of 5%. While this is slightly below the 6% CAGR that we continue to expect between 2020 and 2025, I would remind you that there will be volatility along the way.
Let me give you some detail on our cost and expense guidance.
For Adjusted cost of sales, we are expecting a range of 32.2% to 34.2%. Given that we are now more than 12 months past the launch of Comirnaty, we expect its negative impact on cost of sales margins to be less than it was in 2021, assuming a similar level of revenues. Further, Paxlovid is expected to have a very positive impact on cost of sales as a percent of revenues in 2022.
On Adjusted SI&A, we expect $12.5 to $13.5 billion, an increase of $900 million at the midpoint, as compared to 2021.
In addition, we expect our Adjusted R&D guidance range to be $10.5 to $11.5 billion; at the midpoint, that is about $500 million higher than last year.
We expect an adjusted effective tax rate for the year somewhat higher than 2021 at Approximately 16.0%.
These assumptions yield an Adjusted diluted EPS range of $6.35 to $6.55 or 47% operational growth at the midpoint compared to 2021, excluding an expected $0.06 negative impact from foreign exchange.
I would like to point out some additional information which may be helpful for your models. You will note that our guidance assumes a weighted average share count of approximately 5.8 billion, which represents an increase of approximately 100 million shares over 2021. This accounts for the number of shares that we normally issue for employee compensation annually. The increase of 100 million shares over 2021 decreases our EPS by about 10 cents at the mid-point. I notice that most of your models instead assume a flat share count for 2022 as compared to 2021.
From the first quarter of 2022 and going forward, we've made a decision to modify our adjusted financials' treatment of amortization of intangibles. Previously, we only excluded amortization related to large mergers and acquisitions, but we will now exclude all intangible asset amortization expense. This is anticipated to contribute 6 cents to our 2022 adjusted diluted earnings per share, and helps improve comparability with our peers.
2022 guidance once again assumes no share repurchases. You will note that Pfizer did not repurchase shares in either 2020 or 2021. While we continue to have outstanding unused authorization to repurchase another $5.3 billion of stock and can be opportunistic, given the potentially value-enhancing business development opportunities which are available to us, we do not expect to repurchase shares in 2022.
Now a word on our 32% stake in the Consumer JV with GSK. As you know, GSK has announced its intention to engage in a demerger transaction for at least 80% of its 68% stake in the JV in summer 2022. We talked about our stake as a non-core asset whose value we will seek to realize over time. While we have determined neither the manner nor timing of how we will do so, there are a number of possible alternatives and we will attempt to monetize this asset in the manner which will create the most value for our shareholders. We receive approximately $600 million in pre-tax income from the JV annually, and this will not change as a result of the demerger transaction, and our guidance assumes that this will continue throughout 2022 with no change to our 32% stake.
Let me quickly remind you of some assumptions and context on the projected COVID-19 vaccine contribution and our collaboration agreement:
The Pfizer-BioNTech COVID-19 vaccine collaboration construct is a 50/50 gross profit split.
Pfizer books the vast majority of the global collaboration revenue, except for Germany and Turkey where we receive a profit share from BioNTech, and we do not participate in the China region.
We continue to expect that we can manufacture 4 billion doses in total by the end of 2022.
The $1 billion increase in expected COVID vaccine revenues to approximately $32 billion in 2022 primarily represents the impact of contracts signed since mid-December, which was the cutoff for our prior guidance. While we can’t predict what may be needed due to omicron or other variants, I would also caution you that there is less potential upside to this guidance through the year, compared to the situation we faced in 2021 when the vaccine was newly available and few people had received any doses of the vaccine.
As you will remember, our cost of sales for the COVID-19 vaccine revenue includes manufacturing and distribution costs, applicable royalty expenses, and a payment to BioNTech representing the 50% gross profit split.
We expect that the Adjusted income before tax margin for the COVID-19 vaccine contribution to be slightly higher than the high 20's as a percentage of revenue that we had in 2021.
Unlike the situation for Comirnaty, demand for Paxlovid should have upside from these levels, depending on the outcomes of discussions with certain governments and potential purchases for stockpiling against future coronavirus pandemics.
If we remove the projected COVID-19 vaccine and Paxlovid contribution from both periods, you will see that we expect the 2022 revenue range to be $45 to $47 billion, representing approximately 5 percent operational revenue growth at the midpoint.
Please remember our guidance excludes the former revenue contribution of approximately $300 million for Meridian, and all 2021 quarters have been recast to exclude Meridian as discontinued operations, accounting for its divestiture.
Going forward, we will not give earnings guidance excluding the estimated income from our Comirnaty direct sales and alliance revenues and Paxlovid. [However, to help you with your forecasting, a couple of minutes ago, I gave you my view on 2022 Comirnaty pre-tax margins. For Paxlovid, I would think about its margins as being typical for a small molecule drug, and unlike Comirnaty, it is expected to not be dilutive to pre-tax margins. To help you further, several years ago before COVID-19 existed, I spoke about our business being on a path back to a 40% plus pre-tax margin and we expect to achieve this level in 2022 for the business excluding Comirnaty direct sales and alliance revenues and Paxlovid.]
[Slide 45: Capital Allocation Framework]
And going forward we will continue to be prudent in our capital allocation activities with the opportunities for deployment shown here on this slide.
[Slide 46: Key Takeaways]
In summary, an exceptionally strong quarter and year, based on continued strong performance for our growth drivers. During the year, we raised guidance, and for the year, we met or exceeded our guidance in all key metrics. Our pipeline continues to advance, and we have invested [record amounts] to support that advance. Last week, Arena's shareholders voted to approve Pfizer's acquisition of the company. We look forward to a targeted closing of the Arena acquisition as soon as the first half of 2022, subject to the satisfaction of the closing conditions, including antitrust approvals. We continue to expect to be active in regards to business development throughout 2022, as we continue to get access to the best external science and bring breakthroughs to patients in 2025 and beyond.
With that, let me turn it over to Chris to start the Q&A Session.
Disclosure Notice: This material represents prepared remarks for Pfizer Inc.’s earnings conference call and is not an official transcript. Except where otherwise noted, the information contained in these prepared remarks is as of February 8, 2022. We assume no obligation to update any forward-looking statements contained in these prepared remarks as a result of new information or future events or developments.
These prepared remarks contain forward-looking statements about, among other topics, our anticipated operating and financial performance; reorganizations; business plans and prospects; expectations for our product pipeline, in-line products and product candidates, including anticipated regulatory submissions, data read-outs, study starts, approvals, clinical trial results and other developing data, revenue contribution, growth, performance, timing of exclusivity and potential benefits; strategic reviews; capital allocation objectives; dividends and share repurchases; plans for and prospects of our acquisitions, dispositions and other business development activities, and our ability to successfully capitalize on these opportunities; manufacturing and product supply; our efforts to respond to COVID-19, including the Pfizer-BioNTech COVID-19 vaccine (Comirnaty) and our oral COVID-19 treatment (Paxlovid); and our expectations regarding the impact of COVID-19 on our business, operations and financial results that involve substantial risks and uncertainties. You can identify these statements by the fact that they use future dates or use words such as “will,” “may,” “could,” “likely,” “ongoing,” “anticipate,” “estimate,” “expect,” “project,” “intend,” “plan,” “believe,” “assume,” “target,” “forecast,” “guidance,” “goal,” “objective,” “aim,” “seek,” “potential” and other words and terms of similar meaning. Among the factors that could cause actual results to differ materially from past results and future plans and projected future results are the following:
Risks Related to Our Business, Industry and Operations, and Business Development:
• the outcome of research and development (R&D) activities, including, the ability to meet anticipated pre-clinical or clinical endpoints, commencement and/or completion dates for our pre-clinical or clinical trials, regulatory submission dates, and/or regulatory approval and/or launch dates; the possibility of unfavorable pre-clinical and clinical trial results, including the possibility of unfavorable new pre-clinical or clinical data and further analyses of existing pre-clinical or clinical data; the risk that pre-clinical and clinical trial data are subject to differing interpretations and assessments, including during the peer review/publication process, in the scientific community generally, and by regulatory authorities; and whether and when additional data from our pipeline programs will be published in scientific journal publications and, if so, when and with what modifications and interpretations;
• our ability to successfully address comments received from regulatory authorities such as the U.S. Food and Drug Administration or the European Medicines Agency, or obtain approval for new products or indications from regulators on a timely basis or at all; regulatory decisions impacting labeling, including the scope of indicated patient populations, product dosage, manufacturing processes, safety and/or other matters, including decisions relating to emerging developments regarding potential product impurities; the impact of recommendations by technical or advisory committees; and the timing of pricing approvals and product launches;
• claims and concerns that may arise regarding the safety or efficacy of in-line products and product candidates, including claims and concerns that may arise from the outcome of post-approval clinical trials, which could impact marketing approval, product labeling, and/or availability or commercial potential, including uncertainties regarding the commercial or other impact of the results of the Xeljanz ORAL Surveillance (A3921133) study or actions by regulatory authorities based on analysis of ORAL Surveillance or other data, including on other Janus kinase (JAK) inhibitors in our portfolio;
• the success and impact of external business-development activities, including the ability to identify and execute on potential business development opportunities; the ability to satisfy the conditions to closing of announced transactions in the anticipated time frame or at all; the ability to realize the anticipated benefits of any such transactions in the anticipated time frame or at all; the potential need for and impact of additional equity or debt financing to pursue these opportunities, which could result in increased leverage and/or a downgrade of our credit ratings; challenges integrating the businesses and operations; disruption to business and operations relationships; risks related to growing revenues for certain acquired products; significant transaction costs; and unknown liabilities;
• competition, including from new product entrants, in-line branded products, generic products, private label products, biosimilars and product candidates that treat or prevent diseases and conditions similar to those treated or intended to be prevented by our in-line products and product candidates;
• the ability to successfully market both new and existing products, including biosimilars;
• difficulties or delays in manufacturing, sales or marketing; supply disruptions, shortages or stockouts at our facilities or third-party facilities that we rely on; and legal or regulatory actions;
• the impact of public health outbreaks, epidemics or pandemics (such as the COVID-19 pandemic), including the impact of vaccine mandates where applicable, on our business, operations and financial condition and results, including impacts on our employees, manufacturing, supply chain, sales and marketing, research and development and clinical trials;
• risks and uncertainties related to our efforts to develop and commercialize a vaccine to help prevent COVID-19 and an oral COVID-19 treatment, as well as challenges related to their manufacturing, supply and distribution, including, among others, uncertainties inherent in research and development, including the ability to meet anticipated clinical endpoints, commencement and/or completion dates for clinical trials, regulatory submission dates, regulatory approval dates and/or launch dates, as well as risks associated with pre-clinical and clinical data (including the Phase 1/2/3 or Phase 4 data for Comirnaty, any other vaccine candidate in the BNT162 program, Paxlovid or any other future COVID-19 treatment) in any of our studies in pediatrics, adolescents or adults or real world evidence, including the possibility of unfavorable new pre-clinical, clinical or safety data and further analyses of existing pre-clinical, clinical or safety data or further information regarding the quality of pre-clinical, clinical or safety data, including by audit or inspection; the ability to produce comparable clinical or other results for Comirnaty or Paxlovid, including the rate of effectiveness and/or efficacy, safety and tolerability profile observed to date, in additional analyses of the Phase 3 trial for Comirnaty or Paxlovid and additional studies, in real-world data studies or in larger, more diverse populations following commercialization; the ability of Comirnaty or any future vaccine to prevent, or Paxlovid or any other future COVID-19 treatment to be effective against, COVID-19 caused by emerging virus variants; the risk that more widespread use of the vaccine or Paxlovid will lead to new information about efficacy, safety or other developments, including the risk of additional adverse reactions, some of which may be serious; the risk that pre-clinical and clinical trial data are subject to differing interpretations and assessments, including during the peer review/publication process, in the scientific community generally, and by regulatory authorities; whether and when additional data from the BNT162 mRNA vaccine program, Paxlovid or other programs will be published in scientific journal publications and, if so, when and with what modifications and interpretations; whether regulatory authorities will be satisfied with the design of and results from these and any future pre-clinical and clinical studies; whether and when submissions to request emergency use or conditional marketing authorizations for Comirnaty or any potential future vaccines in additional populations, for a booster dose for Comirnaty or any potential future vaccines (including potential future annual boosters or re-vaccinations), and/or biologics license and/or EUA applications or amendments to any such applications may be filed in particular jurisdictions for Comirnaty or any other potential vaccines, and if obtained, whether or when such EUA or licenses will expire or terminate; whether and when submissions to request emergency use or conditional marketing authorizations for Paxlovid or any other future COVID-19 treatment and/or any drug applications for any indication for Paxlovid or any other future COVID-19 treatment may be filed in any jurisdiction, and if obtained, whether or when such EUA or licenses will expire or terminate; whether and when any application that may be pending or filed for Comirnaty, other vaccines that may result from the BNT162 program, Paxlovid or any other future COVID-19 treatment or any other COVID-19 program may be approved by particular regulatory authorities, which will depend on myriad factors, including making a determination as to whether the vaccine’s or drug’s benefits outweigh its known risks and determination of the vaccine’s or drug’s efficacy and, if approved, whether it will be commercially successful; decisions by regulatory authorities impacting labeling or marketing, manufacturing processes, safety and/or other matters that could affect the availability or commercial potential of a vaccine or drug, including development of products or therapies by other companies; disruptions in the relationships between us and our collaboration partners, clinical trial sites or third-party suppliers, including our relationship with BioNTech; the risk that other companies may produce superior or competitive products; the risk that demand for any products may be reduced or no longer exist; the possibility that COVID-19 will diminish in severity or prevalence, or disappear entirely; risks related to the availability of raw materials to manufacture or test any such products; challenges related to our vaccine’s formulation, dosing schedule and attendant storage, distribution and administration requirements, including risks related to storage and handling after delivery by Pfizer; the risk that we may not be able to successfully develop other vaccine formulations, booster doses or potential future annual boosters or re-vaccinations or new variant-specific vaccines; the risk that we may not be able to recoup costs associated with our R&D and manufacturing efforts; risks associated with any changes in the way we approach or provide research funding for the BNT162 program, Paxlovid or any other COVID-19 program; challenges and risks associated with the pace of our development programs; the risk that we may not be able to maintain or scale up manufacturing capacity on a timely basis or maintain access to logistics or supply channels commensurate with global demand for our vaccine or any treatment for COVID-19, which would negatively impact our ability to supply the estimated numbers of doses of our vaccine or treatment courses of Paxlovid within the projected time periods; whether and when additional supply or purchase agreements will be reached; the risk that demand for any products maybe reduced or no longer exist; uncertainties regarding the ability to obtain recommendations from vaccine or treatment advisory or technical committees and other public health authorities and uncertainties regarding the commercial impact of any such recommendations; pricing and access challenges for such products; challenges related to public confidence or awareness of our COVID-19 vaccine or Paxlovid, including challenges driven by misinformation, access, concerns about clinical data integrity and prescriber and pharmacy education; trade restrictions; potential third-party royalties related to our COVID-19 vaccine or Paxlovid; and competitive developments;
• trends toward managed care and healthcare cost containment, and our ability to obtain or maintain timely or adequate pricing or favorable formulary placement for our products;
• interest rate and foreign currency exchange rate fluctuations, including the impact of possible currency devaluations in countries experiencing high inflation rates;
• any significant issues involving our largest wholesale distributors or government customers, which account for a substantial portion of our revenues;
• the impact of the increased presence of counterfeit medicines or vaccines in the pharmaceutical supply chain;
• any significant issues related to the outsourcing of certain operational and staff functions to third parties; and any significant issues related to our JVs and other third-party business arrangements;
• uncertainties related to general economic, political, business, industry, regulatory and market conditions including, without limitation, uncertainties related to the impact on us, our customers, suppliers and lenders and counterparties to our foreign-exchange and interest-rate agreements of challenging global economic conditions and recent and possible future changes in global financial markets;
• any changes in business, political and economic conditions due to actual or threatened terrorist activity, civil unrest or military action;
• the impact of product recalls, withdrawals and other unusual items, including uncertainties related to regulator-directed risk evaluations and assessments;
• trade buying patterns;
• the risk of an impairment charge related to our intangible assets, goodwill or equity-method investments;
• the impact of, and risks and uncertainties related to, restructurings and internal reorganizations, as well as any other corporate strategic initiatives, and cost-reduction and productivity initiatives, each of which requires upfront costs but may fail to yield anticipated benefits and may result in unexpected costs or organizational disruption;
Risks Related to Government Regulation and Legal Proceedings:
• the impact of any U.S. healthcare reform or legislation or any significant spending reductions or cost controls affecting Medicare, Medicaid or other publicly funded or subsidized health programs or changes in the tax treatment of employer-sponsored health insurance that may be implemented;
• U.S. federal or state legislation or regulatory action and/or policy efforts affecting, among other things, pharmaceutical product pricing, intellectual property, reimbursement or access or restrictions on U.S. direct-to-consumer advertising; limitations on interactions with healthcare professionals and other industry stakeholders; as well as pricing pressures for our products as a result of highly competitive insurance markets;
• legislation or regulatory action in markets outside of the U.S., including China, affecting pharmaceutical product pricing, intellectual property, reimbursement or access, including, in particular, continued government-mandated reductions in prices and access restrictions for certain biopharmaceutical products to control costs in those markets;
• the exposure of our operations globally to possible capital and exchange controls, economic conditions, expropriation and other restrictive government actions, changes in intellectual property legal protections and remedies, as well as political unrest, unstable governments and legal systems and inter-governmental disputes;
• legal defense costs, insurance expenses, settlement costs and contingencies, including those related to actual or alleged environmental contamination;
• the risk and impact of an adverse decision or settlement and the adequacy of reserves related to legal proceedings;
• the risk and impact of tax related litigation;
• governmental laws and regulations affecting our operations, including, without limitation, changes in laws and regulations or their interpretation, including, among others, changes in tax laws and regulations internationally and in the U.S., including, among others, potential adoption of global minimum taxation requirements and potential changes to existing tax law by the current U.S. Presidential administration and Congress;
Risks Related to Intellectual Property, Technology and Security:
• any significant breakdown or interruption of our information technology systems and infrastructure (including cloud services);
• any business disruption, theft of confidential or proprietary information, extortion or integrity compromise resulting from a cyber-attack;
• the risk that our currently pending or future patent applications may not be granted on a timely basis or at all, or any patent-term extensions that we seek may not be granted on a timely basis, if at all; and
• our ability to protect our patents and other intellectual property, including against claims of invalidity that could result in loss of exclusivity, unasserted intellectual property claims and in response to any pressure, or legal or regulatory action by, various stakeholders or governments that could potentially result in us not seeking intellectual property protection for or agreeing not to enforce or being restricted from enforcing intellectual property related to our products, including our vaccine to help prevent COVID-19 and our oral COVID-19 treatment.
We cannot guarantee that any forward-looking statement will be realized. Should known or unknown risks or uncertainties materialize or should underlying assumptions prove inaccurate, actual results could vary materially from past results and those anticipated, estimated or projected. Investors are cautioned not to put undue reliance on forward-looking statements. A further list and description of risks, uncertainties and other matters can be found in our Annual Report on Form 10-K for the fiscal year ended December 31, 2020 and in our subsequent reports on Form 10-Q, in each case including in the sections thereof captioned “Forward-Looking Information and Factors That May Affect Future Results” and “Item 1A. Risk Factors,” and in our subsequent reports on Form 8-K.
These prepared remarks include discussion of certain financial measures that were not prepared in accordance with generally accepted accounting principles (GAAP). Reconciliations of those non-GAAP financial measures to the most directly comparable GAAP financial measures can be found in the Company’s Current Report on Form 8-K dated February 8, 2022.
These prepared remarks may include discussion of certain clinical studies relating to various in-line products and/or product candidates. These studies typically are part of a larger body of clinical data relating to such products or product candidates, and the discussion herein should be considered in the context of the larger body of data. In addition, clinical trial data are subject to differing interpretations, and, even when we view data as sufficient to support the safety and/or effectiveness of a product candidate or a new indication for an in-line product, regulatory authorities may not share our views and may require additional data or may deny approval altogether.
Emergency uses of the Pfizer-BioNTech COVID-19 Vaccine and Paxlovid have not been approved or licensed by the FDA. Emergency uses of Comirnaty have been authorized by the FDA, under an Emergency Use Authorization (EUA) to prevent Coronavirus Disease 2019 (COVID-19) in individuals 5 years of age and older. Comirnaty is licensed by the FDA for individuals 16 years of age and older. In addition, Comirnaty is under EUA for individuals ages 12 through 15, a third dose for certain immunocompromised individuals 5 years of age and older, and a booster dose for individuals 12 years of age and older. Paxlovid has been authorized for emergency use by the FDA under an EUA, for the treatment of mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg [88 lbs]) with positive results of direct SARS CoV-2 viral testing, and who are at high-risk for progression to severe COVID-19, including hospitalization or death. The emergency uses are only authorized for the duration of the declaration that circumstances exist justifying the authorization of emergency use of the medical product under Section 564(b)(1) of the FD&C Act unless the declaration is terminated or authorization revoked sooner. Please see the EUA Fact Sheets at www.cvdvaccine-us.com and www.covid19oralrx.com.
The information contained on our website or any third-party website is not incorporated by reference into this earnings release.
⭐️⭐️⭐️⭐️Enjoy thousands of books and journals and videos to improve, educate and thrive in times of yet more change! Organic non toxic lifestyle every day! Independently published by Laurel Sobol— https://www.etsy.com/search?q=laurel%20sobol if book links are broken or no longer available then find books on Amazon. This is the home and supporter sponsor of Organic Lifestyle Today. Join over 8 billion people global in healthy creation of Elohim, our Creator. The timeless manmade Apocalyptic Star Wars with UFO technology, Geo, Weather, Disease Dispersal Warfare against Bene' Qodesh must end forevermore. People must dream, believe, hope. strive for the world and space they know is fantastical, beautiful, exotic, wonderful and miraculous --just the way our great I Am our God made it all. Soli Deo Gloria forever. ⭐️
SO THE PLANDEMIC WAS PLOTTED OUT FOR COVID-19 AND THE COVID-19 VACCINES AS EARLY AS 22 YEARS AGO… HTTP://CITIZENS.NEWS/646061.HTML UNIVERSITY OF OREGON IS BREAKING THE LAW TOO AND MAY FACE CHARGES SUCH AS UNIVERSITY OF TEXAS. UNIVERSITY OF TEXAS ADMITS IT PROBABLY BROKE THE LAW BY PARTNERING WITH WUHAN LAB TO DEVELOP BIOWEAPONS
Who are the mystery people on CDC Independent 15 member panel that approved CDC votes to recommend vaccine for children ages?
October 19, 2022 without regard to Supreme Court Ruling involvement of Illegal COVID Vaccine Mandates and not reviewing the comments and human rights legalities, and the steamrolling CDC genocide agenda…
Looks like Supreme Court Ruling about Not legalizing COVID-19 Vaccine Mandates is being challenged by 15 independent people who voted to add COVID-19 Vaccinations to childhood Vaccination schedules! CDC to Vote on adding COVID-19 Immunization schedule for children in already deadly children’s vaccination schedule❤️🩹‼️
Special note: The numerous people listed cover about one year of services with CDC but not verified as members who voted to change the course of human history and increased genocide of children all ages subjected to massive toxic antigens like MRNA COVID-19 Vaccines.
CDC Web Archive
THIS WEB PAGE IS ARCHIVED FOR HISTORICAL PURPOSES AND IS NO LONGER BEING UPDATED. PLEASE GO TO CDC HOME OR USE THE A-Z INDEX OR SEARCH FOR MORE RECENT INFORMATION.
CDC Home
Search
A-Z Index
Skip directly to site contentSkip directly to page optionsSkip directly to A-Z link
Advisory Committee on Immunization Practices (ACIP)
Section Navigation
ACIP Members August 2021- June 2022
August 23, 2020: Content on this page kept for historical reasons.
Printer friendly version of ACIP Members list pdf icon[9 pages]
The ACIP includes 15 voting members responsible for making vaccine recommendations. The Secretary of the U.S. Department of Health and Human Services (DHHS) selects these members following an application and nomination process. Fourteen of the members have expertise in vaccinology, immunology, pediatrics, internal medicine, nursing, family medicine, virology, public health, infectious diseases, and/or preventive medicine; one member is a consumer representative who provides perspectives on the social and community aspects of vaccination.
In addition to the 15 voting members, ACIP includes 8 ex officio members who represent other federal agencies with responsibility for immunization programs in the United States, and 30 non-voting representatives of liaison organizations that bring related immunization expertise.
Members and representatives serve on the Committee voluntarily.
CHAIR
LEE, Grace M., MD, MPH
Associate Chief Medical Officer for Practice Innovation
Lucile Packard Children’s Hospital
Professor of Pediatrics, Stanford University School of Medicine
Stanford, CA
Term: 8/4/2021 – 6/30/2023
EXECUTIVE SECRETARY
COHN, Amanda, MD
Senior Advisor for Vaccines
National Center for Immunization and Respiratory Diseases
Centers for Disease Control and Prevention
Atlanta, GA
Members
AULT, Kevin A., MD, FACOG, FIDSA
Professor and Division Director
Department of Obstetrics and Gynecology
University of Kansas Medical Center
Kansas City, KS
Term: 10/26/2018 – 6/30/2022
BAHTA, Lynn, RN, MPH, CPH
Immunization Program Clinical Consultant
Infectious Disease, Epidemiology, Prevention & Control Division
Minnesota Department of Health
Saint Paul, Minnesota
Term: 7/1/2019 – 6/30/2023
BELL, Beth P., MD, MPH
Clinical Professor
Department of Global Health, School of Public Health
University of Washington
Seattle, WA
Term: 7/1/2019 – 6/30/2023
CHEN, Wilbur H., MD, MS, FACP, FIDSA
Professor of Medicine
Center for Vaccine Development and Global Health
University of Maryland School of Medicine
Baltimore, MD
Term: 12/23/2020 – 6/30/2024
DALEY, Matthew F., MD
Senior Investigator
Institute for Health Research
Kaiser Permanente Colorado
Aurora, CO
Term: 1/4/2021 – 6/30/2024
KOTTON, Camille Nelson, MD, FIDSA, FAST
Clinical Director, Transplant and Immunocompromised Host Infectious Diseases
Infectious Diseases Division, Massachusetts General Hospital
Associate Professor of Medicine, Harvard Medical School
Boston, MA
Term: 12/23/2020 – 6/30/2024
LONG, Sarah S., MD
Professor of Pediatrics
Drexel University College of Medicine
Section of Infectious Diseases
St. Christopher’s Hospital for Children
Philadelphia, Pennsylvania
Term: 12/24/2020 – 6/30/2024
MCNALLY, Veronica V., JD
President and CEO
Franny Strong Foundation
West Bloomfield, Michigan
Term: 10/31/2018 – 6/30/2022
POEHLING, Katherine A., MD, MPH
Professor of Pediatrics and Epidemiology and Prevention
Director, Pediatric Population Health
Department of Pediatrics
Wake Forest School of Medicine
Winston-Salem, NC
Term: 7/1/2019 – 6/30/2023
SÁNCHEZ, Pablo J., M.D.
Professor of Pediatrics
The Ohio State University – Nationwide Children’s Hospital
Divisions of Neonatal-Perinatal Medicine and Pediatric Infectious Diseases
Director, Clinical & Translational Research (Neonatology)
Center for Perinatal Research
The Research Institute at Nationwide Children’s Hospital
Columbus, Ohio
Term: 7/1/2019 – 6/30/2023
TALBOT, Helen Keipp, MD
Associate Professor of Medicine
Vanderbilt University
Nashville, TN
Term: 10/29/2018 – 6/30/2022
Ex Officio Members
Centers for Medicare and Medicaid Services (CMS)
HANCE, Mary Beth
Senior Policy Advisor
Division of Quality, Evaluations and Health Outcomes
Children and Adults Health Programs Group
Center for Medicaid, CHIP and Survey & Certification
Centers for Medicare and Medicaid Services
Baltimore, MD
Food and Drug Administration (FDA)
FINK, Doran, MD, PhD
Deputy Director, Clinical, Division of Vaccines and Related Products Applications
Office of Vaccines Research and Review
Center for Biologics Evaluation and Research
Food and Drug Administration
Silver Spring, MD
Health Resources and Services Administration (HRSA)
RUBIN, Mary, MD
Chief Medical Officer
Division of Injury Compensation Programs
Rockville, MD
Indian Health Service (IHS)
WEISER, Thomas, MD, MPH
Medical Epidemiologist
Portland Area Indian Health Service
Portland, OR
Office of Infectious Disease and HIV/AIDS Policy (OIDP)
KIM, David, MD, MA
Director, Division of Vaccines, OIDP
Office of the Assistant Secretary for Health
Department of Health and Human Services
Washington, DC
National Institutes of Health (NIH)
BEIGEL, John, M.D.
Associate Director for Clinical Research
Division of Microbiology and Infectious Diseases
National Institute of Allergy and Infectious Diseases (NIAID)
Bethesda, MD
Liaison Representatives
American Academy of Family Physicians (AAFP)
ROCKWELL, Pamela G., D.O.
Associate Professor, Department of Family Medicine,
University of Michigan Medical School
Medical Director, Dominos Farms Family Medicine
Ann Arbor, MI
American Academy of Pediatrics (AAP)
MALDONADO, Yvonne, MD
Senior Associate Dean for Faculty Development and Diversity
Professor of Pediatrics and Health Research and Policy
Chief, Division of Pediatric Infectious Diseases
Stanford University School of Medicine
Stanford, CA
American Academy of Pediatrics (AAP) Red Book Editor
KIMBERLIN, David, MD
Professor of Pediatrics
Division of Pediatric Infectious Diseases
The University of Alabama at Birmingham School of Medicine
Birmingham, AL
American Academy of Physician Assistants (AAPA)
LÉGER, Marie-Michèle, MPH, PA-C
Senior Director, Clinical and Health Affairs
American Academy of Physician Assistants
Alexandria, VA
American College Health Association (ACHA)
CHAI, Thevy S., MD
Director of Medical Services
Campus Health Services
University of North Carolina at Chapel Hill
Chapel Hill, NC
American College Health Association (ACHA) (alternate)
MCMULLEN, Sharon, RN, MPH, FACHA
she/her/hers
Assistant Vice President of Student & Campus Life for Health and Wellbeing
Cornell Health
Ithaca, NY
American College of Nurse Midwives (ACNM)
HAYES, Carol E., CNM, MN, MPH, FACNM
Adjunct Professor
Georgia State University School of Nursing
Atlanta, GA
American College of Nurse Midwives (ACNM) (alternate)
MEHARRY, Pamela M., PHD, CNM
Midwifery Educator, Human Resources for Health
In partnership with University of Rwanda and University of Illinois, Chicago
American College of Obstetricians and Gynecologists (ACOG)
ECKERT, Linda O., MD, FACOG
Professor, Department of Obstetrics & Gynecology
Adjunct Professor, Department of Global Health
University of Washington
Seattle, WA
American College of Physicians (ACP)
GOLDMAN, Jason M. MD, FACP
Affiliate Assistant Professor of Clinical Biomedical Science, Florida Atlantic University, Boca Raton, Florida
Private Practice
Coral Springs, FL
American Geriatrics Society (AGS)
SCHMADER, Kenneth, MD
Professor of Medicine-Geriatrics
Geriatrics Division Chief
Duke University and Durham VA Medical Centers
Durham, NC
America’s Health Insurance Plans (AHIP)
GLUCKMAN, Robert A., MD, MACP
Chief Medical Officer, Providence Health Plans
Beaverton, OR
American Immunization Registry Association (AIRA)
COYLE, Rebecca, MSEd
Executive Director, AIRA
Washington, DC
American Medical Association (AMA)
FRYHOFER, Sandra Adamson, MD
Adjunct Associate Professor of Medicine
Emory University School of Medicine
Atlanta, GA
American Nurses Association (ANA)
RITTLE, Charles (Chad), DNP, MPH, RN
Assistant Professor, Nursing Faculty
Chatham University, School of Health Sciences
Pittsburgh, PA
American Osteopathic Association (AOA)
GROGG, Stanley E., DO
Associate Dean/Professor of Pediatrics
Oklahoma State University-Center for Health Sciences
Tulsa, OK
American Pharmacists Association (APhA)
FOSTER, Stephan L., PharmD
CAPT (Ret) U.S.P.H.S.
Professor, College of Pharmacy
University of Tennessee Health Sciences Center
Memphis, TN
Association of Immunization Managers (AIM)
HOWELL, Molly, MPH
Immunization Program Manager
North Dakota Department of Health
Bismarck, ND
Association for Prevention Teaching and Research (APTR)
McKINNEY, W. Paul, MD
Professor and Associate Dean
University of Louisville School of Public Health and Information Sciences
Louisville, KY
Association of State and Territorial Health Officials (ASTHO)
SHAH, Nirav D., MD, JD
Director
Maine Center for Disease Control and Prevention
Augusta, ME
Biotechnology Industry Organization (BIO)
ARTHUR, Phyllis A., MBA
Senior Director, Vaccines, Immunotherapeutics and Diagnostics Policy
Washington, DC
Council of State and Territorial Epidemiologists (CSTE)
HAHN, Christine, MD
State Epidemiologist
Office of Epidemiology, Food Protection and Immunization
Idaho Department of Health and Welfare
Boise, ID
Council of State and Territorial Epidemiologists (CSTE) (alternate)
LETT, Susan, MD, MPH
Medical Director, Immunization Program
Division of Epidemiology and Immunization
Massachusetts Department of Public Health
Boston, MA
Canadian National Advisory Committee on Immunization (NACI)
QUACH, Caroline, MD, MSc
Pediatric Infectious Disease Specialist and Medical Microbiologist
Medical Lead, Infection Prevention and Control Unit
Medical Co-director – Laboratory Medicine, Optilab
Montreal-CHUM
Montreal, Québec, Canada
Infectious Diseases Society of America (IDSA)
BAKER, Carol J., MD
Professor of Pediatrics
Molecular Virology and Microbiology
Baylor College of Medicine
Houston, TX
International Society for Travel Medicine (ISTM)
BARNETT, Elizabeth D, MD
Professor of Pediatrics
Boston University School of Medicine
Boston, MA
National Association of County and City Health Officials (NACCHO)
ZAHN, Matthew, MD
Medical Director, Epidemiology
Orange County Health Care Agency
Santa Ana, CA
National Association of County and City Health Officials (NACCHO) (alternate)
DUCHIN, Jeffrey, MD
Health Officer and Chief, Communicable Disease Epidemiology and Immunization Section
Public Health – Seattle and King County
Professor in Medicine
Division of Allergy and Infectious Diseases
University of Washington School of Medicine and School of Public Health
Seattle, WA
National Association of Pediatric Nurse Practitioners (NAPNAP)
STINCHFIELD, Patricia A., RN, MS, CPNP
Director
Infectious Disease/Immunology/Infection Control
Children’s Hospitals and Clinics of Minnesota
St. Paul, MN
National Foundation for Infectious Diseases (NFID)
SCHAFFNER, William, MD
Chairman, Department of Preventive Medicine
Vanderbilt University School of Medicine
Nashville, TN
National Foundation for Infectious Diseases (NFID) (alternate)
DALTON, Marla, PE, CAE
Executive Director & CEO
National Foundation for Infectious Diseases (NFID)
Bethesda, MD
National Medical Association (NMA)
WHITLEY-WILLIAMS, Patricia, MD
Professor and Chair
University of Medicine and Dentistry of New Jersey
Robert Wood Johnson Medical School
New Brunswick, NJ
Pediatric Infectious Diseases Society (PIDS)
O’LEARY, Sean, MD, MPH
Associate Professor of Pediatrics
Pediatric Infectious Diseases
General Academic Pediatrics
Children’s Hospital Colorado
University of Colorado School of Medicine
Pediatric Infectious Diseases Society (PIDS) (alternate)
SAWYER, Mark H, MD
Professor of Clinical Pediatrics
University of California, San Diego School of Medicine
San Diego, CA
Pharmaceutical Research and Manufacturers of America (PhRMA)
ROBERTSON, Corey, MD, MPH
Senior Director, US Medical, Sanofi Pasteur
Swiftwater, PA
Society for Adolescent Health and Medicine (SAHM)
MIDDLEMAN, Amy B., MD, MSEd, MPH
Professor of Pediatrics
Chief, Section of Adolescent Medicine
University of Oklahoma Health Sciences Center
Oklahoma City, OK
Society for Healthcare Epidemiology of America (SHEA)
Best Beautiful Books and Journals In The World in the Little House of Miracles Books and Journals many of which are to be found at Barnes and Noble https://www.barnesandnoble.com
. Find Books On YouTube Too
🐥🐥🐥🐥🐥🐥🐥🐥🐥🐥🐥🐥🐥🐥
PREVENTABLE BABY DEATHS! NO IT’S NEVER SAFE TO PUT TOXIC MANMADE SUBSTANCES IN A PREGNANT PERSON!
Irony after millions died from Covid-19 mRNA vaccines globally, many forced to take the toxic payload…Now only if it was and is used for ethical non political and non violent uses regulated by a global highly ethical biblical regulatory commission trusted and honored by Elohim himself. It’s the people the taxpayers who will be covering the costs in every sense of the Word.
Now only if it was and is used for ethical non political and non violent uses regulated by a global highly ethical biblical regulatory commission trusted and honored by Elohim himself. It’s the people the taxpayers who will be covering the costs in every sense of the Word.
Now we have these two people who pop up to receive a global award in science—
Nobel prize for medicine goes to U.S. duo who discovered microRNA
Winner of the 2024 Nobel Prize in medicine is announced
By Niklas Pollard, Ludwig Burger, Jonathan Allen
STOCKHOLM (Reuters) -U.S. scientists Victor Ambros and Gary Ruvkun won the 2024 Nobel Prize in Medicine on Monday for the discovery of microRNA and its crucial role in how multicellular organisms grow and live.
Their work helped explain how cells specialise and develop into different types, such as muscle and nerve cells, even though all the cells in an individual contain the same set of genes and instructions for growing and staying alive.
"The Nobel's, you know, there's a word we use for Major League Baseball, it's called 'The Show'. Which means it's not any show, it's THE show," Ruvkun told Reuters, describing what it was like being thrust into the global spotlight.
He joked that collaborating with Ambros and receiving previous awards meant they had been "joined at the hip for quite a while".
"That's been great. He's a wonderful guy," Ruvkun added by phone. Ambros seconded by saying he was happy to share the award with "a great friend".
The Nobel Assembly, the award-giving body, said in a statement that the laureates discovered a new class of tiny RNA molecules, which play a crucial role in gene regulation.
"Their groundbreaking discovery revealed a completely new principle of gene regulation that turned out to be essential for multicellular organisms, including humans," the assembly said.
Also speaking to Reuters, Ambros described microRNA as a "communication network amongst genes that enables the cells in our bodies to generate all kinds of different complex structures and functions".
Ambros is a professor at the University of Massachusetts Medical School, while Ruvkun is a professor at Harvard Medical School and also affiliated with Massachusetts General Hospital in Boston.
In the late 1980s, Ambros and Ruvkun undertook postdoctorate studies in the laboratory of Robert Horvitz, himself a Nobel Prize winner in 2002, studying a 1 mm long roundworm.
Their discoveries on how certain microRNAs in the roundworm govern growth of organs and tissue was initially dismissed as specific to the species.
More work published by Ruvkun's research group in 2000, however, showed that all animal life had relied on the mechanism for more than 500 million years.
BUILDING BLOCKS FOR LIFE
MicroRNA comes into play when single-strand messenger RNA - the subject of last year's Nobel Prize in medicine - is decoded and translated into making proteins, the building blocks of all human and animal life.
Messenger RNA, or mRNA, in turn, emerges from the universal blueprint in every cell nucleus, the double-helix DNA.
Professor Gunilla Karlsson Hedestam of the Karolinska Institute said that, while the 2023 prize was linked to the specific use in COVID-19 vaccines, this year's award was for a leap in basic understanding with many potential future applications.
Janosch Heller, Assistant Professor in Biomedical Sciences at Dublin City University, who was not involved in selecting the winners, said that the findings had boosted the understanding of diseases such as epilepsy.
The winners of the prize for physiology or medicine are selected by the Nobel Assembly of Sweden's Karolinska Institute medical university and receive a prize sum of 11 million Swedish crowns ($1.1 million).
As in every year, the physiology or medicine prize was the first in the crop of Nobels, arguably the most prestigious prizes in science, literature and humanitarian endeavour, with the remaining five set to be unveiled over the coming days.
Created in the will of Swedish dynamite inventor and businessman Alfred Nobel, the prizes have been awarded for breakthroughs in science, literature and peace since 1901, while economics is a later addition.
Past winners of the Nobel medicine prize include many famous researchers such as Ivan Pavlov in 1904, most known for his experiments on behaviour using dogs, and Alexander Fleming, who shared the 1945 prize for the discovery of penicillin.
Last year's medicine prize was awarded to the runaway favourites Katalin Kariko, a Hungarian scientist, and U.S. colleague Drew Weissman, for discoveries that paved the way for COVID-19 vaccines that helped curb the pandemic.
Steeped in tradition, the science, literature and economics prizes are presented to the laureates in a ceremony on Dec. 10, the anniversary of Alfred Nobel's death, followed by a lavish banquet at Stockholm city hall. Separate festivities attend the winner of the peace prize in Oslo on the same day. ($1 = 10.1086 Swedish crowns)
(Reporting by Niklas Pollard and Johan Ahlander in Stockholm, Ludwig Burger in Frankfurt and Jonathan Allan in New York; additional reporting by Terje Solsvik in Oslo and Anna Ringstrom in Stockholm; editing by Alex Richardson)
🟢🟢🟢🟢🟢🟢🟢🟢🟢🟢🟢🟢🟢🟢
FLASHBACK— WHO REMEMBERS WHEN BARACK HUSSEIN OBAMA WENT TO EUROPE TO LOCATE SPANISH INFLUENZA FROM CORPS DUG UP ESPECIALLY FOR HIM? NOW WITH EXTREME NUMBER OF UKRAINE BIOLABS BORDERING RUSSIA—IT’S CLEAR WHAT WAS GOING ON ADDED TO THE FACT THAT THIS X VARIANT OF COVID-19 IS ENSUING EARLY 2025
WILL IT BEGIN WITH STERILIZATION AND END IN EUTHANASIA? READ THROUGH TO THE END…FEDS COMING AFTER AMERICANS WITH DISABILITIES! AFTER DEMORALIZING, DEHUMANIZING AND VICTIMIZING AMERICAN PEOPLE…
WASHINGTON — President Joe Biden on Thursday issued two executive orders mandating vaccines for federal workers and contractors and announced new requirements for large employers and health care providers that he said would affect around 100 million workers, more than two-thirds of the U.S. workforce.
"We've been patient, but our patience is wearing thin," Biden said, making a direct appeal to the 80 million people who he said were still unvaccinated. "Your refusal has cost all of us."
Biden also announced that he asked the Department of Labor to issue an emergency rule requiring all employers with 100 or more employees to ensure their workforce is fully vaccinated or require any unvaccinated workers to produce a negative Covid test at least once a week. The requirement could carry a $14,000 fine per violation and would affect two-thirds of the country's workforce, a senior administration official said.
Employees working in health care facilities that receive Medicare or Medicaid reimbursement will also be required to be vaccinated, Biden said, a move that will impact 7 million workers at 50,000 health care providers.
UPDATE! NEW MRNA TRIAL ANTIBODY NIRSEVIMAB WILL NULLIFY THE STUDY BECAUSE THE OUTCOME OF MRNA MODERNA VACCINE SIDE EFFECTS WILL BE REDUCED. THE SAME PRINCIPLE OF THEM ADDING HEART ANTI-INFLAMMATION DRUGS TO SUBDUE COVID-19 REACTIONS TO THE VACCINE. THE COVID-19 MRNA VACCINES SIDE EFFECTS ARE GREATER IN ALL RESPECTS THAN WITHOUT MRNA.
New mRNA trial Antibody nirsevimab will nullify the study because the outcome of mRNA Moderna vaccine side effects will be reduced. The same principle of them adding heart anti-inflammation drugs to subdue Covid-19 reactions to the vaccine. The Covid-19 mRNA vaccines side effects are greater in all respects than without mRNA.
Sugar Can Turn Off Biological Healthy Metrics Likened To Covid-19 Spike Proteins That Turn Off T-Cells That Protect The Immune System To Wage Sleuth Silent Killer Bioweapon Nanoparticles That Emit Light Flashes To Communicate To Each Other mRNA System Wide —By Trojan Horse
























































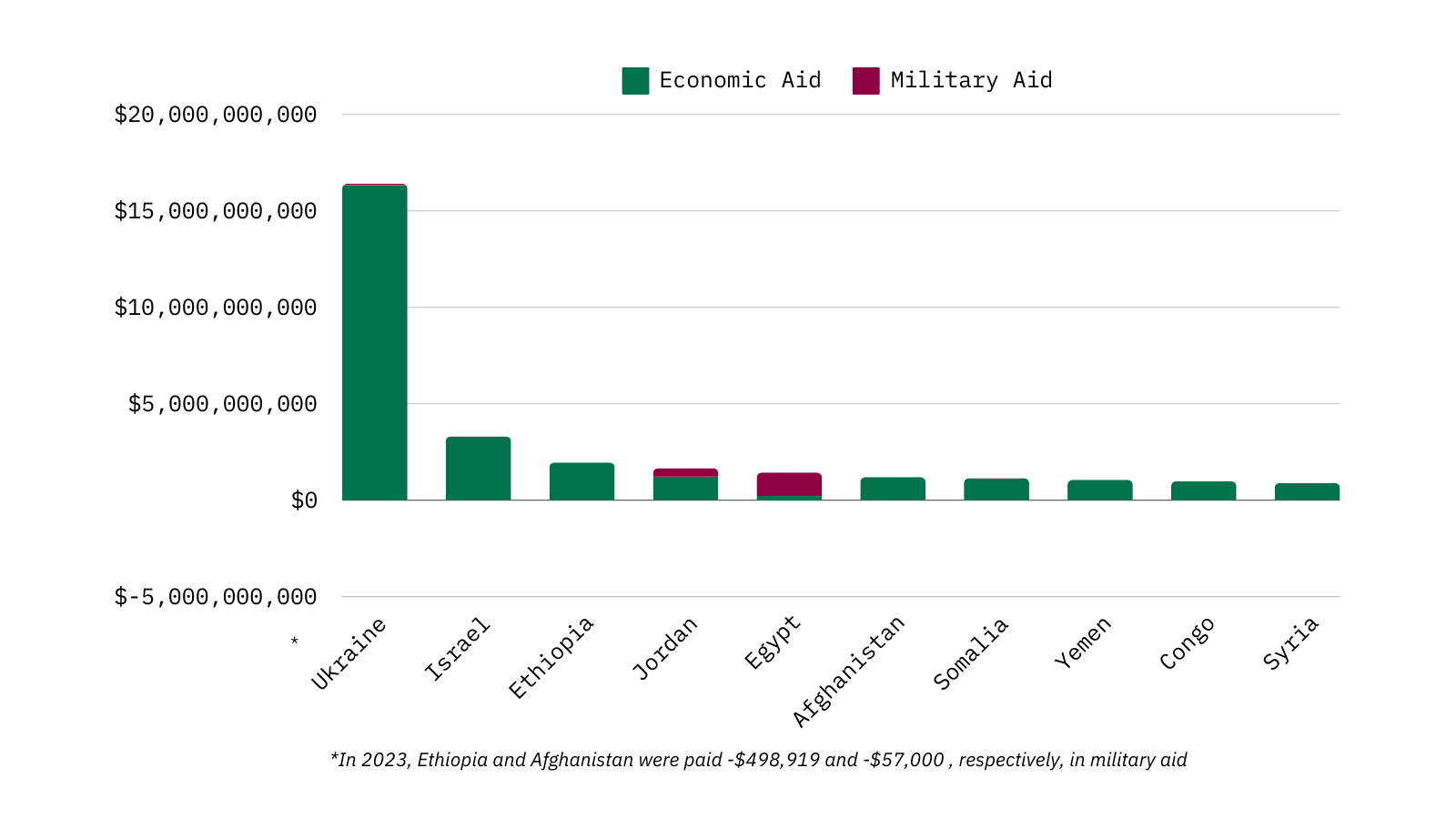
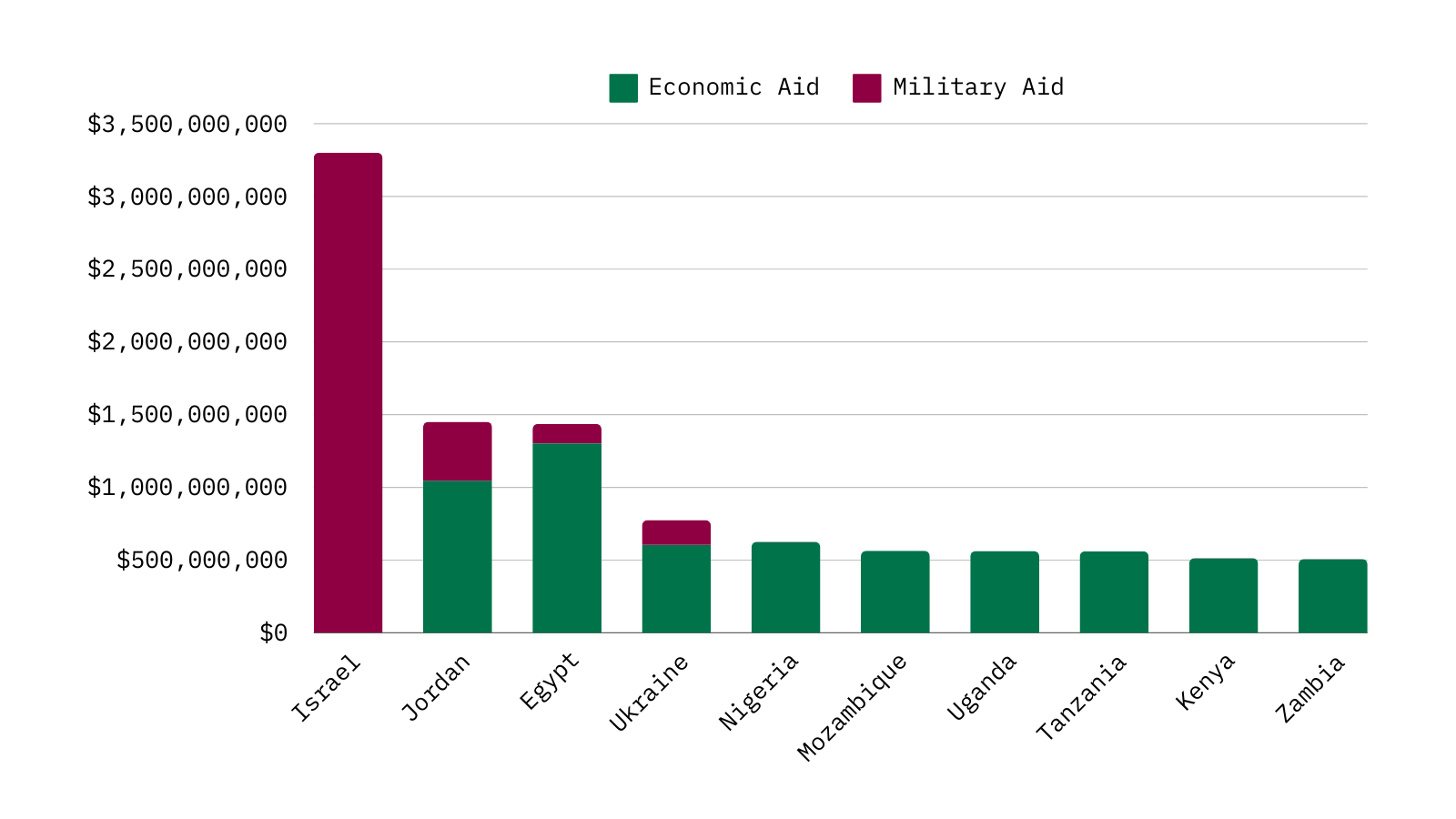
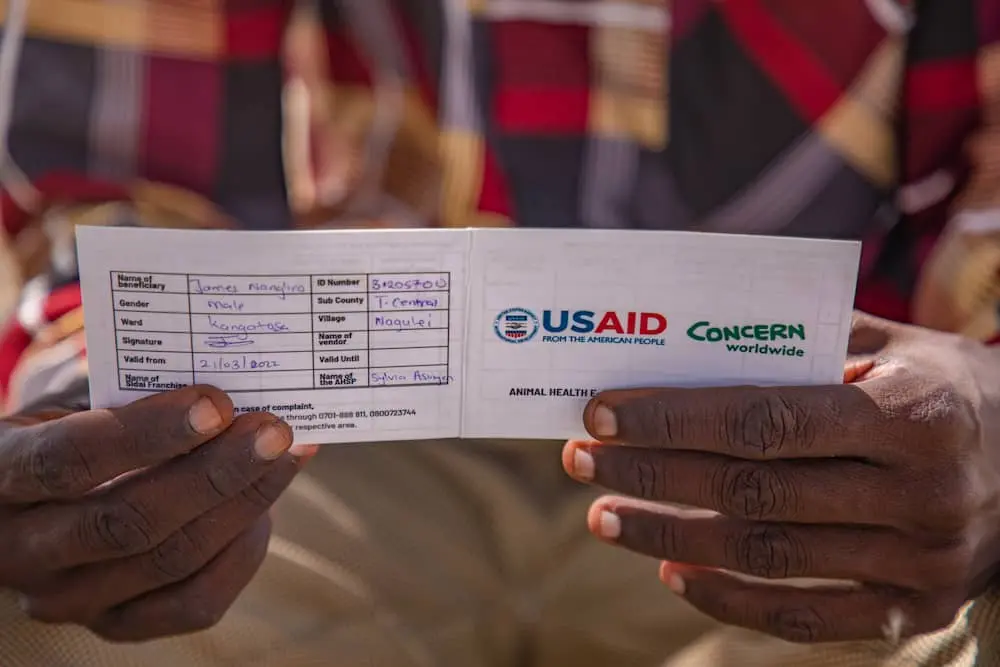






























Comments